
This post is also available in: Nederlands (Dutch)
One, because of the quotes, slightly longer blog:
In the field of target group transport and aids supply, a budget reduction spiral has been in place for years. If you think the bottom has been reached, it turns out it can still be lower. Meanwhile, far too late, the quay seems to be turning the ship around.
Taxi companies
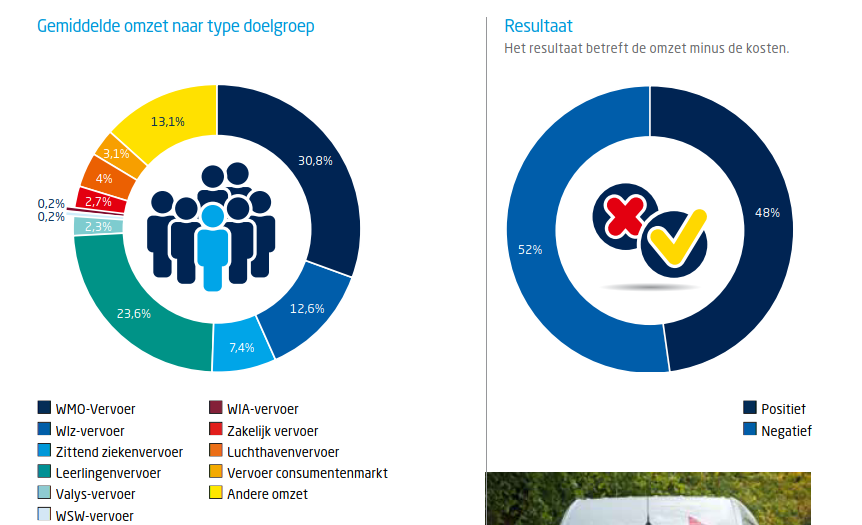
Panteia investigated the taxi market in 2017. They found, among other things, that more than three quarters of transport is target group transport. If margins nearly turn out to exist and 52 of the taxi companies write red figures, then that is quite worrying and alarming:
Wheelchair transport tenders increasingly not awarded
Hopefully, the bottom has been reached with transport tenders
It is scraping over the bottom in order to be able to earn a living in the target group transport. Especially now during the Corona crisis.
Municipalities
Clients such as municipalities also face budget cuts and extra tasks. Very easily a Catch 22 situation is created. A dance to be able to realize transport and aids for as little budget as possible. From the updated handout of purchasing aids:
“2.1 Make sure the client’s need is in the picture
Having a good picture of the purchasing needs for a procurement process is of great importance for the successful purchase of WMO tools. What is purchased by the municipality must meet the needs of the different types of users in the municipality. Below are the most important qualitative and quantitative data that should be in the picture.
Quantitative data:
a How many users use aids and how large is the target group with a complex care demand?
b What aids are used, what is the number of aids in use per product category, the number of deliveries and intakes in the current year per product category?
c What developments have been in the last few years, for example changes in financial contribution of the user, the design of collective pools of aids?
d What developments in aids use are expected for the future, for example on the basis of demographics, technology or government policy?
………
Qualitative data:
a What are users satisfied with and what problems do they experience in the provision and use of aids?
b What delivery time and quality of service and maintenance do users think is reasonable?
c What service is expected of the supplier in addition to providing aids?
d What can be done by the supplier in consultation with the users, without the intervention or approval of the municipality? “
Is that the aids user in the picture? Turnover figures and general satisfaction survey and throwing the contact with the user over the fence? How appropriate can an aid then be? How can the municipality assess whether a possible individual complaint is justified?
Health insurance
Health insurers struggle with costs and efficiency of resources in relation to quality. A study by NIVEL and VU shows:
“2.3.8 After cutting back now time for quality
Health insurers feel their responsibility over the safe application of devices. They would “like to keep their finger on the pulse.” At the same time, they indicate that it is difficult for them to implement this. Especially since they don’t really know how to do it. “Going to visit every week is not an option”. Health insurers indicate that they cannot be the main institution responsible for medical and technical content. Health insurers have an important role in costs and indicate that the bottom has been reached when it comes to reducing the cost of purchasing medical devices. For example, where €50 million was spent on incontinence three years ago, that is now €40 million. According to health insurers, now it is a matter of guaranteeing quality and services. The costs may be slightly higher, but health insurers do not think anything is wrong with that. A health insurer illustrates: “What we have achieved above all is that the high margins of suppliers but also of manufacturers are edged. Because it’s not our job to cut users short.”
The question, of course, is whether that bottom should be reached first, so that there is no longer a margin for quality among companies. Only then to focus on quality. A quality that an insurer itself indicates is difficult to implement safe application of devices.
For the elderly among us: That looks a bit like Dik Trom who sits backwards on an unwilling donkey, and pulls at its tail…. (Dutch children’s book)

It’s great if you can stay in the saddle in such a situation as a aids provider, taxi company or health care provider.
Dots on the horizon?
The NIVEL and VU report contains a lot of policy language and dots on the horizon. Remember that quality assurance may require a different direction. Then those dots that you have previously put in your field of view on the horizon are less useful.
Delivering quality against everything else, is that sustainable?
If companies want to offer quality, but have to wait and see if this is appreciated in the tender? If they are wondering if there is still work for everyone in the coming period. How can you cope with that? If quality does not work on the basis of trust in a long-term sustainable contract relationship but has to be fought again every few years against health insurers and municipalities? How can you then continue to deliver structural quality? What are the costs of always changing companies, new vehicles, other drivers, in the case of a new contract? And the old, not yet depreciated vehicles, isn’t that capital destruction?
I admire companies and municipalities that manage to ensure that quality and care for passengers and employees are leading!
Aids vendors
There are only a few very large companies left in the provision of aids. In addition to a number of smaller (sub)contractors, manufacturers often have a specific target area.
Red figures are also written at these large companies:
Again, wheelchair supplier Welzorg is losing.
What does keeping in the air an actually too big to fail aids company cost? What investment was made by the municipalities in the hulpmiddelencentrum new owner? Why did we let it come to this?
The aids user and passenger
Disastrous for the aids user! It is not surprising that, among other things, the patient federation finds that the quality of the care system needs to be improved:
“The consequences for people who are dealing with a malfunctioning or ill-fitting aid are great. They can sometimes literally no longer go onto the street, can’t go to school or work and miss contacts outside the door. In October, six organisations, including the Patient Federation, wrote a letter to the House of Representatives. Veldman: ‘We highlight two key problems in that letter. Firstly, more attention should be paid to aid care. For example, the word aid already sounds small, as if a medicine is more important and you can do without a aid. But an aid is absolutely essential to people’s lives. And secondly, there should be more choices for people. To put it bluntly, people get the cheapest stuff by default in some places. The supply is very scant in some areas.’ “
That, for example, in Sweden, it can be very different from a guest blog by Sandra Zwagerman on troostoverleven.nl: Wheelchair Valhalla. Act quickly and appropriately.
Black figures important for quality
Only a company that writes structurally black figures is able to make from the profit quality to one of the foundations of its existence, in addition to survival, customer and employee satisfaction. This is in the fibres of a company that is set up according to the Rhineland management model. That’s where you can offer a structurally sound solution and stay alive!
In tender rounds, no race to the bottom fits. One period in full swing, the period after you have to you lay off your employees because you were a little too expensive. Promote quality, how?
Or health insurers with quality indicators, which they are essentially not, but which do lead to additional stifling regulatory burdens:
Administrative burden costs nursing home care 25,000 fte. :
“Experiences from the corona crisis offer opportunities
Reduction of administrative burdens starts with confidence, Berenschot writes in her report. Something that the Public Health Council noted earlier in its report‘Token of confidence’. The current situation offers opportunities.”
The situation in which the hospitals and insurers are in a state of struggle with each other who will pay the additional costs in the face of the Corona crisis, offers little hope of a rapid recovery of working on the basis of trust. That it is already thought that the care deferred by Covid19 might not be a sensible care, shows a particular thought squirm among insurers.
No Anglo-Saxon model managers fit in, but municipal officials and health insurance workers with sufficient substantive knowledge of care, resources and taxi transport do fit. A contract is not “Awarded” for nothing!
Give people and companies the space to offer quality. It’s really high time for a big system and paradigm change. Many costs go into ineffective control, regulation, procurement, advice and lawsuits.
Money that can also be invested in quality, in addition to providing confidence!