This post is also available in:
Nederlands ( Dutch)
One, because of the quotes, slightly longer blog:
In the field of target group transport and aids supply, a budget reduction spiral has been in place for years. If you think the bottom has been reached, it turns out it can still be lower. Meanwhile, far too late, the quay seems to be turning the ship around.
Taxi companies
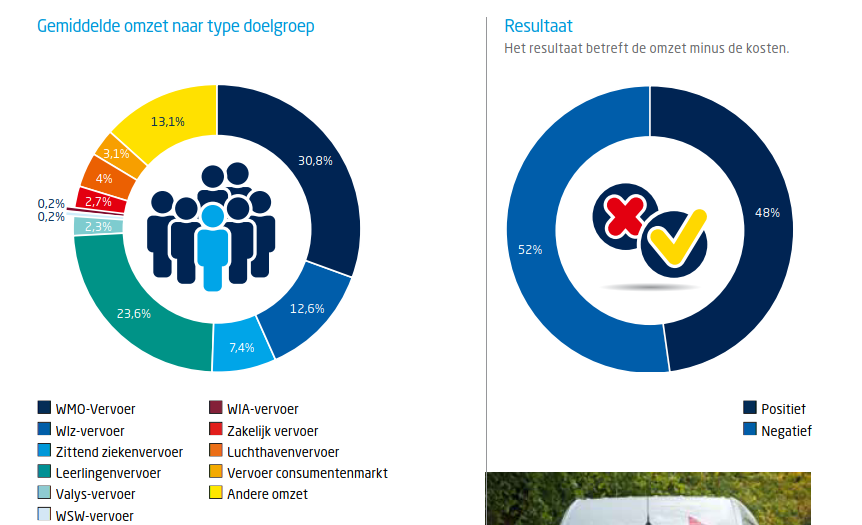
Panteia investigated the taxi market in 2017. They found, among other things, that more than three quarters of transport is target group transport. If margins nearly turn out to exist and 52 of the taxi companies write red figures, then that is quite worrying and alarming:
Distribution in audiences and the result Wheelchair transport tenders increasingly not awarded
Hopefully, the bottom has been reached with transport tenders
It is scraping over the bottom in order to be able to earn a living in the target group transport. Especially now during the Corona crisis.
Municipalities
Clients such as municipalities also face budget cuts and extra tasks. Very easily a Catch 22 situation is created. A dance to be able to realize transport and aids for as little budget as possible. From the updated handout of purchasing aids:
“2.1 Make sure the client’s need is in the picture Quantitative data: Qualitative data:
Is that the aids user in the picture? Turnover figures and general satisfaction survey and throwing the contact with the user over the fence? How appropriate can an aid then be? How can the municipality assess whether a possible individual complaint is justified?
Health insurance
Health insurers struggle with costs and efficiency of resources in relation to quality. A study by NIVEL and VU shows:
“2.3.8 After cutting back now time for quality
The question, of course, is whether that bottom should be reached first, so that there is no longer a margin for quality among companies. Only then to focus on quality. A quality that an insurer itself indicates is difficult to implement safe application of devices.
Dik Trom on the donkey (source: petrOlly flickr.com CC BY-NC-ND 2.0) It’s great if you can stay in the saddle in such a situation as a aids provider, taxi company or health care provider.
Dots on the horizon?
The NIVEL and VU report contains a lot of policy language and dots on the horizon. Remember that quality assurance may require a different direction. Then those dots that you have previously put in your field of view on the horizon are less useful.
Delivering quality against everything else, is that sustainable?
If companies want to offer quality, but have to wait and see if this is appreciated in the tender? If they are wondering if there is still work for everyone in the coming period. How can you cope with that? If quality does not work on the basis of trust in a long-term sustainable contract relationship but has to be fought again every few years against health insurers and municipalities? How can you then continue to deliver structural quality? What are the costs of always changing companies, new vehicles, other drivers, in the case of a new contract? And the old, not yet depreciated vehicles, isn’t that capital destruction?
Aids vendors
There are only a few very large companies left in the provision of aids. In addition to a number of smaller (sub)contractors, manufacturers often have a specific target area.
Again, wheelchair supplier Welzorg is losing.
Hulpmiddelencentrum bankrupt, wheelchairs and mobility scooters remain with clients for the time being.
What does keeping in the air an actually too big to fail aids company cost? What investment was made by the municipalities in the hulpmiddelencentrum new owner? Why did we let it come to this?
The aids user and passenger
Disastrous for the aids user! It is not surprising that, among other things, the patient federation finds that the quality of the care system needs to be improved:
“The consequences for people who are dealing with a malfunctioning or ill-fitting aid are great. They can sometimes literally no longer go onto the street, can’t go to school or work and miss contacts outside the door. In October, six organisations, including the Patient Federation, wrote a letter to the House of Representatives. Veldman: ‘We highlight two key problems in that letter. Firstly, more attention should be paid to aid care. For example, the word aid already sounds small, as if a medicine is more important and you can do without a aid. But an aid is absolutely essential to people’s lives. And secondly, there should be more choices for people. To put it bluntly, people get the cheapest stuff by default in some places. The supply is very scant in some areas.’ “
That, for example, in Sweden, it can be very different from a guest blog by Sandra Zwagerman on troostoverleven.nl: Wheelchair Valhalla. Act quickly and appropriately.
Black figures important for quality
Only a company that writes structurally black figures is able to make from the profit quality to one of the foundations of its existence, in addition to survival, customer and employee satisfaction. This is in the fibres of a company that is set up according to the Rhineland management model. That’s where you can offer a structurally sound solution and stay alive!
Or health insurers with quality indicators, which they are essentially not, but which do lead to additional stifling regulatory burdens:
Administrative burden costs nursing home care 25,000 fte
“Experiences from the corona crisis offer opportunities Reduction of administrative burdens starts with confidence, Berenschot writes in her report. Something that the Public Health Council noted earlier in its report‘Token of confidence’.
The situation in which the hospitals and insurers are in a state of struggle with each other who will pay the additional costs in the face of the Corona crisis, offers little hope of a rapid recovery of working on the basis of trust. That it is already thought that the care deferred by Covid19 might not be a sensible care, shows a particular thought squirm among insurers.
No Anglo-Saxon model managers fit in, but municipal officials and health insurance workers with sufficient substantive knowledge of care, resources and taxi transport do fit. A contract is not “Awarded” for nothing!
Give people and companies the space to offer quality. It’s really high time for a big system and paradigm change. Many costs go into ineffective control, regulation, procurement, advice and lawsuits.
Linked to
References
{6637697:K7DPE4N3};{6637697:RW8R7K3E};{6637697:7EJW6ULX};{6637697:SR4PIVZF};{6637697:T4BN3KBH};{6637697:JQVJFMKI};{6637697:KA2SJPGT};{6637697:FV65CGHD};{6637697:DWV4FAVZ};{6637697:BGBRZ9EY};{6637697:7VBJVLRB}
modern-language-association
default
asc
0
950
%7B%22status%22%3A%22success%22%2C%22updateneeded%22%3Afalse%2C%22instance%22%3Afalse%2C%22meta%22%3A%7B%22request_last%22%3A100%2C%22request_next%22%3A50%2C%22used_cache%22%3Atrue%7D%2C%22data%22%3A%5B%7B%22key%22%3A%22H6QK8H8Y%22%2C%22library%22%3A%7B%22id%22%3A6637697%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22SFM%22%2C%22parsedDate%22%3A%222019%22%2C%22numChildren%22%3A1%7D%2C%22bib%22%3A%22%3Cdiv%20class%3D%5C%22csl-bib-body%5C%22%20style%3D%5C%22line-height%3A%202%3B%20padding-left%3A%202em%3B%20text-indent%3A-2em%3B%5C%22%3E%5Cn%20%20%3Cdiv%20class%3D%5C%22csl-entry%5C%22%3ESFM.%20%3Ci%3ECode%20VVR%20Editie%202017.%3C%5C%2Fi%3E%20Sociaal%20Fonds%20Mobiliteit%2C%20mei%202019%2C%20%3Ca%20href%3D%27https%3A%5C%2F%5C%2Fwww.sfmobiliteit.nl%5C%2Fapplication%5C%2Ffiles%5C%2F9415%5C%2F5800%5C%2F7553%5C%2FCode_VVR_Editie_2017_Versie_2.0_mei_2019_def.pdf%27%3Ehttps%3A%5C%2F%5C%2Fwww.sfmobiliteit.nl%5C%2Fapplication%5C%2Ffiles%5C%2F9415%5C%2F5800%5C%2F7553%5C%2FCode_VVR_Editie_2017_Versie_2.0_mei_2019_def.pdf%3C%5C%2Fa%3E.%3C%5C%2Fdiv%3E%5Cn%3C%5C%2Fdiv%3E%22%2C%22data%22%3A%7B%22itemType%22%3A%22document%22%2C%22title%22%3A%22Code%20VVR%20Editie%202017.%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22name%22%3A%22SFM%22%7D%5D%2C%22abstractNote%22%3A%22%22%2C%22date%22%3A%22mei%202019%22%2C%22language%22%3A%22nl%22%2C%22url%22%3A%22https%3A%5C%2F%5C%2Fwww.sfmobiliteit.nl%5C%2Fapplication%5C%2Ffiles%5C%2F9415%5C%2F5800%5C%2F7553%5C%2FCode_VVR_Editie_2017_Versie_2.0_mei_2019_def.pdf%22%2C%22collections%22%3A%5B%224EUQP96T%22%2C%22DD8I76K6%22%5D%2C%22dateModified%22%3A%222020-06-03T08%3A37%3A39Z%22%7D%7D%2C%7B%22key%22%3A%22NXQ22BQW%22%2C%22library%22%3A%7B%22id%22%3A6637697%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22Vocht%20et%20al.%22%2C%22parsedDate%22%3A%222016-07-06%22%2C%22numChildren%22%3A0%7D%2C%22bib%22%3A%22%3Cdiv%20class%3D%5C%22csl-bib-body%5C%22%20style%3D%5C%22line-height%3A%202%3B%20padding-left%3A%202em%3B%20text-indent%3A-2em%3B%5C%22%3E%5Cn%20%20%3Cdiv%20class%3D%5C%22csl-entry%5C%22%3EVocht%2C%20Sven%20de%2C%20et%20al.%20%3Ci%3ELead%20companies%3A%20van%20familiebedrijf%20tot%20multinational%3C%5C%2Fi%3E.%20Lannoo%20Meulenhoff%20-%20Belgium%2C%202016.%3C%5C%2Fdiv%3E%5Cn%3C%5C%2Fdiv%3E%22%2C%22data%22%3A%7B%22itemType%22%3A%22book%22%2C%22title%22%3A%22Lead%20companies%3A%20van%20familiebedrijf%20tot%20multinational%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Sven%20de%22%2C%22lastName%22%3A%22Vocht%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Nadia%22%2C%22lastName%22%3A%22Werkers%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Rudy%22%2C%22lastName%22%3A%22Martens%22%7D%5D%2C%22abstractNote%22%3A%22Vlaamse%20industrie%20zet%20de%20krijtlijnen%20uit%20Vlaamse%20koplopers%20in%20industrieel%20ondernemen%20Onze%20industrie%20ondergaat%20fundamentele%20veranderingen.%20Een%20diversere%20marktvraag%20en%20de%20exponenti%5Cu00eble%20groei%20van%20data%2C%20nieuwe%20software%20en%20hoogtechnologische%20producten%20maken%20onze%20bedrijfsvoering%20steeds%20complexer.%20Lead%20Companies%20banen%20hun%20weg%20door%20dat%20veranderende%20landschap%20en%20cre%5Cu00ebren%20vooruitgang%20met%20een%20vernieuwende%20aanpak.%20De%20Lead%20Company%20zet%20daarbij%20zelf%20belangrijke%20langetermijntrends%20en%20overwint%20zo%20de%20concurrentiedruk.%20Dit%20boek%20bundelt%20de%20ervaring%20en%20inzichten%20van%20vijftig%20executives%20uit%20de%20Vlaamse%20industrie.%20Via%20hun%20getuigenissen%20biedt%20Lead%20Companies%20inspiratie%20voor%20ondernemers%20om%20internationaal%20een%20vooraanstaande%20positie%20te%20kunnen%20innemen.%20Dit%20boek%20beschrijft%20op%20inspirerende%20wijze%20de%20cultuuromslag%20die%20nodig%20is%20om%20de%20transformatie%20van%20onze%20industrie%20vorm%20te%20geven%20en%20de%20toekomst%20van%20onze%20productiebedrijven%20veilig%20te%20stellen.%20Jo%20De%20Backer%2C%20CEO%20Niko%20Group%20Lead%20Companies%20beschrijft%20hoe%20Vlaamse%20kmo%5Cu2019s%20doorgroeien%20tot%20succesvolle%20wereldspelers.%20Vlaamse%20ondernemers%20hebben%20wereldklasse.%20Met%20de%20juiste%20competenties%20in%20huis%20kunnen%20ze%20dromen%20waarmaken.%20Chris%20Van%20Doorslaer%2C%20CEO%20Cartamundi%20%26%20Trends%20Manager%20van%20het%20Jaar%22%2C%22date%22%3A%222016-07-06%22%2C%22language%22%3A%22nl%22%2C%22ISBN%22%3A%229789401436687%22%2C%22url%22%3A%22%22%2C%22collections%22%3A%5B%5D%2C%22dateModified%22%3A%222020-06-02T20%3A22%3A23Z%22%7D%7D%2C%7B%22key%22%3A%228TL88AJ9%22%2C%22library%22%3A%7B%22id%22%3A6637697%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22Vries%22%2C%22parsedDate%22%3A%222019-08-22%22%2C%22numChildren%22%3A1%7D%2C%22bib%22%3A%22%3Cdiv%20class%3D%5C%22csl-bib-body%5C%22%20style%3D%5C%22line-height%3A%202%3B%20padding-left%3A%202em%3B%20text-indent%3A-2em%3B%5C%22%3E%5Cn%20%20%3Cdiv%20class%3D%5C%22csl-entry%5C%22%3EVries%2C%20Judith%20F.%20A.%20de.%20%3Ci%3EDe%20toekomst%20van%20de%20%26%23x2018%3Bopen%26%23x2019%3B%20ambtenaar%3C%5C%2Fi%3E.%20Universiteit%20Utrcht%2C%20Faculteit%20Rebo%2C%2022%20Aug.%202019.%3C%5C%2Fdiv%3E%5Cn%3C%5C%2Fdiv%3E%22%2C%22data%22%3A%7B%22itemType%22%3A%22document%22%2C%22title%22%3A%22De%20toekomst%20van%20de%20%5Cu2018open%5Cu2019%20ambtenaar%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Judith%20F.A.%20de%22%2C%22lastName%22%3A%22Vries%22%7D%5D%2C%22abstractNote%22%3A%22%22%2C%22date%22%3A%2222%20augustus%2C%202019%22%2C%22language%22%3A%22nl%22%2C%22url%22%3A%22%22%2C%22collections%22%3A%5B%22DD8I76K6%22%5D%2C%22dateModified%22%3A%222020-06-01T20%3A45%3A52Z%22%7D%7D%2C%7B%22key%22%3A%22FMQXC4BH%22%2C%22library%22%3A%7B%22id%22%3A6637697%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22Koninkrijksrelaties%22%2C%22parsedDate%22%3A%221990%22%2C%22numChildren%22%3A0%7D%2C%22bib%22%3A%22%3Cdiv%20class%3D%5C%22csl-bib-body%5C%22%20style%3D%5C%22line-height%3A%202%3B%20padding-left%3A%202em%3B%20text-indent%3A-2em%3B%5C%22%3E%5Cn%20%20%3Cdiv%20class%3D%5C%22csl-entry%5C%22%3EKoninkrijksrelaties%2C%20Ministerie%20van%20Binnenlandse%20Zaken%20en.%20%3Ci%3EReglement%20verkeersregels%20en%20verkeerstekens%201990%20%28RVV%201990%29%3C%5C%2Fi%3E.%201990%2C%20%3Ca%20href%3D%27https%3A%5C%2F%5C%2Fwetten.overheid.nl%5C%2FBWBR0004825%5C%2F2020-01-01%5C%2F%23HoofdstukII_Paragraaf27_Artikel59%27%3Ehttps%3A%5C%2F%5C%2Fwetten.overheid.nl%5C%2FBWBR0004825%5C%2F2020-01-01%5C%2F%23HoofdstukII_Paragraaf27_Artikel59%3C%5C%2Fa%3E.%3C%5C%2Fdiv%3E%5Cn%3C%5C%2Fdiv%3E%22%2C%22data%22%3A%7B%22itemType%22%3A%22webpage%22%2C%22title%22%3A%22Reglement%20verkeersregels%20en%20verkeerstekens%201990%20%28RVV%201990%29%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Ministerie%20van%20Binnenlandse%20Zaken%20en%22%2C%22lastName%22%3A%22Koninkrijksrelaties%22%7D%5D%2C%22abstractNote%22%3A%22Reglement%20verkeersregels%20en%20verkeerstekens%201990%20%28RVV%201990%29%22%2C%22date%22%3A%221990%22%2C%22url%22%3A%22https%3A%5C%2F%5C%2Fwetten.overheid.nl%5C%2FBWBR0004825%5C%2F2020-01-01%5C%2F%23HoofdstukII_Paragraaf27_Artikel59%22%2C%22language%22%3A%22nl%22%2C%22collections%22%3A%5B%224EUQP96T%22%2C%22DD8I76K6%22%5D%2C%22dateModified%22%3A%222020-05-30T14%3A09%3A48Z%22%7D%7D%2C%7B%22key%22%3A%22XW7RK762%22%2C%22library%22%3A%7B%22id%22%3A6637697%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22Orton%22%2C%22parsedDate%22%3A%222019-07-05%22%2C%22numChildren%22%3A4%7D%2C%22bib%22%3A%22%3Cdiv%20class%3D%5C%22csl-bib-body%5C%22%20style%3D%5C%22line-height%3A%202%3B%20padding-left%3A%202em%3B%20text-indent%3A-2em%3B%5C%22%3E%5Cn%20%20%3Cdiv%20class%3D%5C%22csl-entry%5C%22%3EOrton%2C%20Nicole%20R.%20%3Ci%3ERide%20Safe%20Brochures%3C%5C%2Fi%3E.%20University%20of%20Michigan%20Transportation%20Research%20Institute%20%28UMTRI%29%2C%205%20July%202019%2C%20%3Ca%20href%3D%27http%3A%5C%2F%5C%2Fwc-transportation-safety.umtri.umich.edu%5C%2Fridesafe-brochure%27%3Ehttp%3A%5C%2F%5C%2Fwc-transportation-safety.umtri.umich.edu%5C%2Fridesafe-brochure%3C%5C%2Fa%3E.%3C%5C%2Fdiv%3E%5Cn%3C%5C%2Fdiv%3E%22%2C%22data%22%3A%7B%22itemType%22%3A%22document%22%2C%22title%22%3A%22Ride%20Safe%20Brochures%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Nicole%20R.%22%2C%22lastName%22%3A%22Orton%22%7D%5D%2C%22abstractNote%22%3A%22%22%2C%22date%22%3A%227-5-2019%20%28en%29%22%2C%22language%22%3A%22en%2C%20sp%2C%20fr%22%2C%22url%22%3A%22http%3A%5C%2F%5C%2Fwc-transportation-safety.umtri.umich.edu%5C%2Fridesafe-brochure%22%2C%22collections%22%3A%5B%22DD8I76K6%22%5D%2C%22dateModified%22%3A%222020-05-30T13%3A08%3A04Z%22%7D%7D%2C%7B%22key%22%3A%22H9N5HE4M%22%2C%22library%22%3A%7B%22id%22%3A6637697%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22Schneider%20et%20al.%22%2C%22parsedDate%22%3A%222016-07%22%2C%22numChildren%22%3A1%7D%2C%22bib%22%3A%22%3Cdiv%20class%3D%5C%22csl-bib-body%5C%22%20style%3D%5C%22line-height%3A%202%3B%20padding-left%3A%202em%3B%20text-indent%3A-2em%3B%5C%22%3E%5Cn%20%20%3Cdiv%20class%3D%5C%22csl-entry%5C%22%3ESchneider%2C%20Lawrence%20W.%2C%20et%20al.%20%3Ci%3EWheelchair%20Occupant%20Studies%3C%5C%2Fi%3E.%20Final%20Report%2C%202016%26%23x2013%3B8%2C%20University%20of%20Michigan%20Transportation%20Research%20Institute%20%28UMTRI%29%2C%20July%202016%2C%20p.%20199%2C%20%3Ca%20href%3D%27https%3A%5C%2F%5C%2Fwww.nhtsa.gov%5C%2Fsites%5C%2Fnhtsa.dot.gov%5C%2Ffiles%5C%2Fumtri-2016-8-wheelchairoccupantstudies.pdf%27%3Ehttps%3A%5C%2F%5C%2Fwww.nhtsa.gov%5C%2Fsites%5C%2Fnhtsa.dot.gov%5C%2Ffiles%5C%2Fumtri-2016-8-wheelchairoccupantstudies.pdf%3C%5C%2Fa%3E.%3C%5C%2Fdiv%3E%5Cn%3C%5C%2Fdiv%3E%22%2C%22data%22%3A%7B%22itemType%22%3A%22report%22%2C%22title%22%3A%22Wheelchair%20Occupant%20Studies%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Lawrence%20W.%22%2C%22lastName%22%3A%22Schneider%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Miriam%22%2C%22lastName%22%3A%22Manary%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Nicole%20R.%22%2C%22lastName%22%3A%22Orton%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Jingwen%20H.%22%2C%22lastName%22%3A%22Hu%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Kathleen%20D.%22%2C%22lastName%22%3A%22Klinich%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Carol%20A.%22%2C%22lastName%22%3A%22Flannagan%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Jamie%20L.%22%2C%22lastName%22%3A%22Moore%22%7D%5D%2C%22abstractNote%22%3A%22The%20goal%20of%20this%20project%20was%20to%20improve%20transportation%20safety%20for%20occupants%20of%20motor%20vehicles%20seated%20in%20wheelchairs%20%28i.e.%2C%20to%5Cnimprove%20wheelchair%20transportation%20safety%2C%20or%20WTS%29%2C%20with%20an%20emphasis%20on%20drivers%20seated%20in%20wheelchairs.%20Investigation%20of%5Cncrash%20and%20non-crash%20events%20involving%20one%20or%20more%20occupants%20in%20wheelchairs%20indicates%20that%20a%20primary%20reason%20occupants%20in%5Cnwheelchairs%20sustain%20serious-to-fatal%20injuries%20is%20improper%20or%20incomplete%20use%20of%20lap%5C%2Fshoulder-belt%20restraints%20due%2C%20in%20large%20part%2C%20to%20%5Cninterference%20by%20wheelchair%20arm%20supports%20with%20proper%20belt%20positioning.%20Efforts%20to%20improve%20frontal%20crash%20protection%20for%20drivers%5Cnin%20wheelchairs%20resulted%20in%20a%20prototype%20seat-belt%20deployment%20system%20%28SBDS%29%20that%20provides%20components%20needed%20to%20complete%20the%5Cnvehicle%20lap%5C%2Fshoulder%20belt%20for%20use%20in%20a%20passive%20mode%20while%20eliminating%20obstacles%20that%20interfere%20with%20maneuvering%20a%20wheelchair%5Cninto%20the%20driver%20space.%20%20Sled-test%20evaluations%20and%20design%20improvements%20of%20a%20commercially%20available%20vehicle-anchored%20head-%5Cnand-back%20restraint%20for%20rear-impact%20protection%20of%20drivers%20in%20wheelchairs%20led%20to%20several%20design%20and%20material%20changes%20that%5Cnimproved%20performance%20and%20that%20the%20manufacturer%20can%20use%20to%20improve%20the%20commercial%20system.%20Results%20of%20sled%20tests%20and%20%5Cncomputer%20simulations%20of%20drivers%20in%20wheelchairs%20with%20and%20without%20steering-wheel%20air-bag%20deployments%20during%20a%2048-kph%20frontal%5Cncrash%20indicate%20that%20there%20is%20little%20basis%20for%20concern%20that%20advanced%20steering-wheel%20air%20bags%20will%20cause%20serious%20injuries%20in%20frontal%5Cncrashes.%20Rather%2C%20steering-wheel%20air%20bags%20almost%20always%20reduce%20the%20risk%20of%20head%2C%20neck%2C%20and%20chest%20injuries.%20Deactivating%5Cnsteering-wheel%20air%20bags%20should%20only%20be%20considered%20when%20the%20driver%20in%20a%20wheelchair%20is%20positioned%20with%20his%5C%2Fher%20chest%20or%20chin%5Cn200%20cm%20or%20less%20from%20the%20air-bag%20module%20during%20normal%20operation%20of%20the%20vehicle.%20Using%20a%20fixed%20upper%20shoulder-belt%20anchor%5Cnpoint%20instead%20of%20the%20OEM%20seat-belt%20retractor%20will%20reduce%20driver%20movement%20toward%20the%20airbag%20module%20during%20pre-impact%20%5Cnbraking%20and%20may%20enhance%20safety%20for%20many%20drivers%20in%20wheelchairs%20by%20providing%20greater%20torso%20stability%20in%20their%20optimal%20posture.%5CnSafety%20Tip%20Sheets%20and%20a%20DriveSafe%20brochure%20have%20been%20developed%20to%20provide%20vehicle%20modifiers%20and%20other%20key%20stakeholder%5Cnwith%20information%20on%20how%20to%20provide%20safer%20transportation%20for%20occupants%20seated%20in%20wheelchairs.%20These%20are%20being%20made%5Cnavailable%20on%20a%20new%20UMTRI%20website%20that%20provides%20a%20wide%20range%20of%20educational%20materials%20on%20WTS%2C%20including%20lists%20of%5Cnwheelchairs%2C%20wheelchair%20tiedown%20and%20occupant%20restraint%20systems%20%28WTORS%29%2C%20and%20wheelchair%20seating%20systems%20that%20comply%5Cnwith%20WTS%20industry%20standards.%20Additional%20work%20is%20needed%20to%20implement%20the%20SBDS%20into%20a%20commercial%20product%20and%20to%20continue%5Cnefforts%20to%20educate%20key%20stakeholder%20groups%20with%20regard%20to%20best%20practice%20in%20WTS%20and%20their%20role%20in%20improving%20transportation%5Cnsafety%20for%20passengers%20and%20drivers%20seated%20in%20wheelchairs.%22%2C%22reportNumber%22%3A%222016-8%22%2C%22reportType%22%3A%22Final%20Report%22%2C%22institution%22%3A%22University%20of%20Michigan%20Transportation%20Research%20Institute%20%28UMTRI%29%22%2C%22date%22%3A%22july%202016%22%2C%22language%22%3A%22en%22%2C%22url%22%3A%22https%3A%5C%2F%5C%2Fwww.nhtsa.gov%5C%2Fsites%5C%2Fnhtsa.dot.gov%5C%2Ffiles%5C%2Fumtri-2016-8-wheelchairoccupantstudies.pdf%22%2C%22collections%22%3A%5B%22DD8I76K6%22%5D%2C%22dateModified%22%3A%222020-05-30T12%3A47%3A48Z%22%7D%7D%2C%7B%22key%22%3A%22GHC5EZ82%22%2C%22library%22%3A%7B%22id%22%3A6637697%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22ISO%22%2C%22parsedDate%22%3A%222008%22%2C%22numChildren%22%3A0%7D%2C%22bib%22%3A%22%3Cdiv%20class%3D%5C%22csl-bib-body%5C%22%20style%3D%5C%22line-height%3A%202%3B%20padding-left%3A%202em%3B%20text-indent%3A-2em%3B%5C%22%3E%5Cn%20%20%3Cdiv%20class%3D%5C%22csl-entry%5C%22%3EISO.%20%3Ci%3EISO%207176-19%3A2008%20%2B%20A1%3A2015.%20Wheelchairs-Wheeled%20Mobility%20Devices%20for%20Use%20as%20Seats%20in%20Motorvehicles%3C%5C%2Fi%3E.%20ISO%2C%202008.%3C%5C%2Fdiv%3E%5Cn%3C%5C%2Fdiv%3E%22%2C%22data%22%3A%7B%22itemType%22%3A%22document%22%2C%22title%22%3A%22ISO%207176-19%3A2008%20%2B%20A1%3A2015.%20Wheelchairs-Wheeled%20mobility%20devices%20for%20use%20as%20seats%20in%20motorvehicles%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22name%22%3A%22ISO%22%7D%5D%2C%22abstractNote%22%3A%22%22%2C%22date%22%3A%222008%22%2C%22language%22%3A%22en%22%2C%22url%22%3A%22%22%2C%22collections%22%3A%5B%224EUQP96T%22%2C%22DD8I76K6%22%5D%2C%22dateModified%22%3A%222020-05-30T11%3A40%3A13Z%22%7D%7D%2C%7B%22key%22%3A%22QR6MY4FR%22%2C%22library%22%3A%7B%22id%22%3A6637697%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22Wij%20zien%20je%20wel%22%2C%22parsedDate%22%3A%222020%22%2C%22numChildren%22%3A1%7D%2C%22bib%22%3A%22%3Cdiv%20class%3D%5C%22csl-bib-body%5C%22%20style%3D%5C%22line-height%3A%202%3B%20padding-left%3A%202em%3B%20text-indent%3A-2em%3B%5C%22%3E%5Cn%20%20%3Cdiv%20class%3D%5C%22csl-entry%5C%22%3EWij%20zien%20je%20wel.%20%3Ci%3EOnderweg%20van%20overleven%20naar%20leven.%20Eindrapport%20en%20aanbevelingen%20werkgroep%20Wij%20zien%20je%20Wel.%3C%5C%2Fi%3E%20Wie%20zien%20je%20wel%2C%20maart%202020%2C%20%3Ca%20href%3D%27https%3A%5C%2F%5C%2Fwww.wijzienjewel.nl%5C%2Fproducten%5C%2Frapport-onderweg-van-overleven-naar-leven%27%3Ehttps%3A%5C%2F%5C%2Fwww.wijzienjewel.nl%5C%2Fproducten%5C%2Frapport-onderweg-van-overleven-naar-leven%3C%5C%2Fa%3E.%3C%5C%2Fdiv%3E%5Cn%3C%5C%2Fdiv%3E%22%2C%22data%22%3A%7B%22itemType%22%3A%22document%22%2C%22title%22%3A%22Onderweg%20van%20overleven%20naar%20leven.%20Eindrapport%20en%20aanbevelingen%20werkgroep%20Wij%20zien%20je%20Wel.%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22%22%2C%22lastName%22%3A%22Wij%20zien%20je%20wel%22%7D%5D%2C%22abstractNote%22%3A%22%22%2C%22date%22%3A%2212%20maart%202020%22%2C%22language%22%3A%22nl%22%2C%22url%22%3A%22https%3A%5C%2F%5C%2Fwww.wijzienjewel.nl%5C%2Fproducten%5C%2Frapport-onderweg-van-overleven-naar-leven%22%2C%22collections%22%3A%5B%224EUQP96T%22%2C%22DD8I76K6%22%5D%2C%22dateModified%22%3A%222020-05-30T11%3A24%3A35Z%22%7D%7D%2C%7B%22key%22%3A%22KY42ICVG%22%2C%22library%22%3A%7B%22id%22%3A6637697%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22Songer%20et%20al.%22%2C%22parsedDate%22%3A%222004-09-13%22%2C%22numChildren%22%3A1%7D%2C%22bib%22%3A%22%3Cdiv%20class%3D%5C%22csl-bib-body%5C%22%20style%3D%5C%22line-height%3A%202%3B%20padding-left%3A%202em%3B%20text-indent%3A-2em%3B%5C%22%3E%5Cn%20%20%3Cdiv%20class%3D%5C%22csl-entry%5C%22%3ESonger%2C%20Thomas%20J.%2C%20et%20al.%20%3Ci%3EThe%20Injury%20Risk%20to%20Wheelchair%20Occupants%20Using%20Motor%20Vehicle%20Transportation%3C%5C%2Fi%3E.%20Sept.%202004%2C%20pp.%20115%26%23x2013%3B29.%3C%5C%2Fdiv%3E%5Cn%3C%5C%2Fdiv%3E%22%2C%22data%22%3A%7B%22itemType%22%3A%22journalArticle%22%2C%22title%22%3A%22The%20Injury%20Risk%20to%20Wheelchair%20Occupants%20Using%20Motor%20Vehicle%20Transportation%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Thomas%20J%22%2C%22lastName%22%3A%22Songer%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Shirley%20G%22%2C%22lastName%22%3A%22Fitzgerald%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Katherine%20A%22%2C%22lastName%22%3A%22Rotko%22%7D%5D%2C%22abstractNote%22%3A%22The%20transportation%20safety%20experience%20for%20persons%20using%20wheelchairs%20is%20largely%20unknown.%20Motor%20vehicle%20crash%20involvement%20and%20injury%20frequency%20was%20examined%20in%20a%20telephone%20interview%20completed%20by%20596%20wheelchair%20users.%20Overall%2C%2042%25%20were%20drivers.%20Most%20subjects%20also%20rode%20as%20passengers%20in%20private%20vehicles%20%2887%25%29%20and%20public%20vehicles%20%2861%25%29.%20Wheelchair%20use%20as%20a%20seat%20in%20the%20vehicle%20was%20higher%20among%20passengers%20than%20drivers.%20Crash%20involvement%20was%20highest%20among%20drivers%20and%20lower%20in%20passengers.%20Reported%20injuries%20from%20non-crash%20scenarios%2C%20though%2C%20were%20higher%20in%20passengers%20compared%20to%20drivers.%20Persons%20seated%20in%20wheelchairs%20in%20vehicles%20appear%20to%20be%20at%20a%20greater%20safety%20risk.%22%2C%22date%22%3A%22September%2013-15%2C%202004%22%2C%22language%22%3A%22en%22%2C%22DOI%22%3A%22%22%2C%22ISSN%22%3A%22%22%2C%22url%22%3A%22%22%2C%22collections%22%3A%5B%224EUQP96T%22%5D%2C%22dateModified%22%3A%222020-05-30T09%3A44%3A45Z%22%7D%7D%2C%7B%22key%22%3A%22H3Q9H333%22%2C%22library%22%3A%7B%22id%22%3A6637697%7D%2C%22meta%22%3A%7B%22parsedDate%22%3A%221997-06-01%22%2C%22numChildren%22%3A1%7D%2C%22bib%22%3A%22%3Cdiv%20class%3D%5C%22csl-bib-body%5C%22%20style%3D%5C%22line-height%3A%202%3B%20padding-left%3A%202em%3B%20text-indent%3A-2em%3B%5C%22%3E%5Cn%20%20%3Cdiv%20class%3D%5C%22csl-entry%5C%22%3E%26%23x201C%3BTravelling%20in%20Vehicles%20While%20in%20a%20Wheelchair%3A%20Joint%20Committee%20on%20Mobility%20for%20Disabled%20People.%26%23x201D%3B%20%3Ci%3EPhysiotherapy%3C%5C%2Fi%3E%2C%20vol.%2083%2C%20no.%206%2C%20June%201997%2C%20p.%20305%2C%20%3Ca%20href%3D%27http%3A%5C%2F%5C%2Fdoi.org%5C%2F10.1016%5C%2FS0031-9406%2805%2966180-9%27%3Ehttp%3A%5C%2F%5C%2Fdoi.org%5C%2F10.1016%5C%2FS0031-9406%2805%2966180-9%3C%5C%2Fa%3E.%3C%5C%2Fdiv%3E%5Cn%3C%5C%2Fdiv%3E%22%2C%22data%22%3A%7B%22itemType%22%3A%22journalArticle%22%2C%22title%22%3A%22Travelling%20in%20Vehicles%20While%20in%20a%20Wheelchair%3A%20Joint%20Committee%20on%20Mobility%20for%20Disabled%20People%22%2C%22creators%22%3A%5B%5D%2C%22abstractNote%22%3A%22Introduction%5CnThe%20safety%20of%20wheelchair%20users%20remaining%20seated%20in%20their%20wheelchairs%20while%20travelling%20in%20vehicles%20such%20as%20social%20services%20minibuses%2C%20Dial-a-Ride%20and%20disability%20organisation%20transportation%20has%20recently%20caused%20considerable%20concern.%20Wheelchair%20manufacturers%20have%20become%20increasingly%20worried%20about%20their%20products%20being%20used%20as%20vehicle%20seats%2C%20for%20which%2C%20in%20the%20past%2C%20they%20were%20never%20designed%2C%20and%20in%20particular%20about%20their%20product%20liability%20in%20the%20case%20of%20an%20accident.%20The%20Department%20of%20Transport%20is%20working%20with%20wheelchair%20manufacturers%20and%20restraint%20manufacturers%20in%20order%20to%20improve%20the%20situation%20in%20the%20future.%20In%20the%20meantime%20there%20are%20examples%20of%20transportation%20groups%20being%20unwilling%20to%20take%20wheelchair%20users%20sitting%20in%20their%20wheelchairs%20and%20as%20a%20result%20disabled%20people%27s%20lives%20are%20liable%20to%20become%20more%20restricted.%22%2C%22date%22%3A%22June%201%2C%201997%22%2C%22language%22%3A%22en%22%2C%22DOI%22%3A%2210.1016%5C%2FS0031-9406%2805%2966180-9%22%2C%22ISSN%22%3A%220031-9406%22%2C%22url%22%3A%22http%3A%5C%2F%5C%2Fwww.sciencedirect.com%5C%2Fscience%5C%2Farticle%5C%2Fpii%5C%2FS0031940605661809%22%2C%22collections%22%3A%5B%224EUQP96T%22%2C%22DD8I76K6%22%5D%2C%22dateModified%22%3A%222020-05-30T09%3A44%3A41Z%22%7D%7D%2C%7B%22key%22%3A%22DV5A8J9B%22%2C%22library%22%3A%7B%22id%22%3A6637697%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22MBA%20et%20al.%22%2C%22parsedDate%22%3A%222012-06-01%22%2C%22numChildren%22%3A0%7D%2C%22bib%22%3A%22%3Cdiv%20class%3D%5C%22csl-bib-body%5C%22%20style%3D%5C%22line-height%3A%202%3B%20padding-left%3A%202em%3B%20text-indent%3A-2em%3B%5C%22%3E%5Cn%20%20%3Cdiv%20class%3D%5C%22csl-entry%5C%22%3EMBA%2C%20Karen%20L.%20Frost%20PhD%2C%20et%20al.%20%26%23x201C%3BWheeled%20Mobility%20Device%20Transportation%20Safety%20in%20Fixed%20Route%20and%20Demand-Responsive%20Public%20Transit%20Vehicles%20within%20the%20United%20States.%26%23x201D%3B%20%3Ci%3EAssistive%20Technology%3C%5C%2Fi%3E%2C%20vol.%2024%2C%20no.%202%2C%20June%202012%2C%20pp.%2087%26%23x2013%3B101%2C%20%3Ca%20href%3D%27http%3A%5C%2F%5C%2Fdoi.org%5C%2F10.1080%5C%2F10400435.2012.659325%27%3Ehttp%3A%5C%2F%5C%2Fdoi.org%5C%2F10.1080%5C%2F10400435.2012.659325%3C%5C%2Fa%3E.%3C%5C%2Fdiv%3E%5Cn%3C%5C%2Fdiv%3E%22%2C%22data%22%3A%7B%22itemType%22%3A%22journalArticle%22%2C%22title%22%3A%22Wheeled%20Mobility%20Device%20Transportation%20Safety%20in%20Fixed%20Route%20and%20Demand-Responsive%20Public%20Transit%20Vehicles%20within%20the%20United%20States%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Karen%20L.%20Frost%20PhD%22%2C%22lastName%22%3A%22MBA%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Linda%20van%22%2C%22lastName%22%3A%22Roosmalen%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Gina%20Bertocci%20PhD%22%2C%22lastName%22%3A%22PE%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Douglas%20J.%22%2C%22lastName%22%3A%22Cross%22%7D%5D%2C%22abstractNote%22%3A%22An%20overview%20of%20the%20current%20status%20of%20wheelchair%20transportation%20safety%20in%20fixed%20route%20and%20demand-responsive%2C%20non-rail%2C%20public%20transportation%20vehicles%20within%20the%20US%20is%20presented.%20A%20description%20of%20each%20mode%20of%20transportation%20is%20provided%2C%20followed%20by%20a%20discussion%20of%20the%20primary%20issues%20affecting%20safety%2C%20accessibility%2C%20and%20usability.%20Technologies%20such%20as%20lifts%2C%20ramps%2C%20securement%20systems%2C%20and%20occupant%20restraint%20systems%2C%20along%20with%20regulations%20and%20voluntary%20industry%20standards%20have%20been%20implemented%20with%20the%20intent%20of%20improving%20safety%20and%20accessibility%20for%20individuals%20who%20travel%20while%20seated%20in%20their%20wheeled%20mobility%20device%20%28e.g.%2C%20wheelchair%20or%20scooter%29.%20However%2C%20across%20both%20fixed%20route%20and%20demand-responsive%20transit%20systems%20a%20myriad%20of%20factors%20such%20as%20nonuse%20and%20misuse%20of%20safety%20systems%2C%20oversized%20wheeled%20mobility%20devices%2C%20vehicle%20space%20constraints%2C%20and%20inadequate%20vehicle%20operator%20training%20may%20place%20wheeled%20mobility%20device%20%28WhMD%29%20users%20at%20risk%20of%20injury%20even%20under%20non-impact%20driving%20conditions.%20Since%20WhMD-related%20incidents%20also%20often%20occur%20during%20the%20boarding%20and%20alighting%20process%2C%20the%20frequency%20of%20these%20events%2C%20along%20with%20factors%20associated%20with%20these%20events%20are%20described%20for%20each%20transit%20mode.%20Recommendations%20for%20improving%20WhMD%20transportation%20are%20discussed%20given%20the%20current%20state%20of%20knowledge.%22%2C%22date%22%3A%22June%201%2C%202012%22%2C%22language%22%3A%22%22%2C%22DOI%22%3A%2210.1080%5C%2F10400435.2012.659325%22%2C%22ISSN%22%3A%221040-0435%22%2C%22url%22%3A%22https%3A%5C%2F%5C%2Fdoi.org%5C%2F10.1080%5C%2F10400435.2012.659325%22%2C%22collections%22%3A%5B%224EUQP96T%22%5D%2C%22dateModified%22%3A%222020-05-30T09%3A44%3A31Z%22%7D%7D%2C%7B%22key%22%3A%22GPU8BK75%22%2C%22library%22%3A%7B%22id%22%3A6637697%7D%2C%22meta%22%3A%7B%22numChildren%22%3A1%7D%2C%22bib%22%3A%22%3Cdiv%20class%3D%5C%22csl-bib-body%5C%22%20style%3D%5C%22line-height%3A%202%3B%20padding-left%3A%202em%3B%20text-indent%3A-2em%3B%5C%22%3E%5Cn%20%20%3Cdiv%20class%3D%5C%22csl-entry%5C%22%3E%3Ci%3E80-20%20Regel%20%7C%20Het%20Effectieve%20Werken%3C%5C%2Fi%3E.%20%3Ca%20href%3D%27https%3A%5C%2F%5C%2Fwww.heteffectievewerken.nl%5C%2Fveelgestelde-vragen%5C%2F80-20-regel.html%27%3Ehttps%3A%5C%2F%5C%2Fwww.heteffectievewerken.nl%5C%2Fveelgestelde-vragen%5C%2F80-20-regel.html%3C%5C%2Fa%3E.%20Accessed%2026%20May%202020.%3C%5C%2Fdiv%3E%5Cn%3C%5C%2Fdiv%3E%22%2C%22data%22%3A%7B%22itemType%22%3A%22webpage%22%2C%22title%22%3A%2280-20%20regel%20%7C%20Het%20Effectieve%20Werken%22%2C%22creators%22%3A%5B%5D%2C%22abstractNote%22%3A%22%22%2C%22date%22%3A%22%22%2C%22url%22%3A%22https%3A%5C%2F%5C%2Fwww.heteffectievewerken.nl%5C%2Fveelgestelde-vragen%5C%2F80-20-regel.html%22%2C%22language%22%3A%22%22%2C%22collections%22%3A%5B%224EUQP96T%22%2C%22DD8I76K6%22%5D%2C%22dateModified%22%3A%222020-05-30T08%3A59%3A21Z%22%7D%7D%2C%7B%22key%22%3A%22T4BN3KBH%22%2C%22library%22%3A%7B%22id%22%3A6637697%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22Mol%20et%20al.%22%2C%22parsedDate%22%3A%222017%22%2C%22numChildren%22%3A1%7D%2C%22bib%22%3A%22%3Cdiv%20class%3D%5C%22csl-bib-body%5C%22%20style%3D%5C%22line-height%3A%202%3B%20padding-left%3A%202em%3B%20text-indent%3A-2em%3B%5C%22%3E%5Cn%20%20%3Cdiv%20class%3D%5C%22csl-entry%5C%22%3EMol%2C%20T.%20I.%2C%20et%20al.%20%3Ci%3EKwaliteitsborging%20van%20extramurale%20medische%20hulpmiddelen%3A%20een%20rolverkenning%20van%20gebruikers%20van%20medische%20hulpmiddelen%2C%20zorgverzekeraars%2C%20gemeenten%20en%20de%20Inspectie%20voor%20de%20Gezondheidszorg%20en%20Jeugd.%3C%5C%2Fi%3E%202017%2C%20p.%2044%2C%20%3Ca%20href%3D%27http%3A%5C%2F%5C%2Fwww.onderzoekpatientveiligheid.nl%27%3Ehttp%3A%5C%2F%5C%2Fwww.onderzoekpatientveiligheid.nl%3C%5C%2Fa%3E.%20%26%23xA9%3B2017%20APH%20research%20Instituut.%3C%5C%2Fdiv%3E%5Cn%3C%5C%2Fdiv%3E%22%2C%22data%22%3A%7B%22itemType%22%3A%22report%22%2C%22title%22%3A%22Kwaliteitsborging%20van%20extramurale%20medische%20hulpmiddelen%3A%20een%20rolverkenning%20van%20gebruikers%20van%20medische%20hulpmiddelen%2C%20zorgverzekeraars%2C%20gemeenten%20en%20de%20Inspectie%20voor%20de%20Gezondheidszorg%20en%20Jeugd.%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22T%20I%22%2C%22lastName%22%3A%22Mol%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22L%22%2C%22lastName%22%3A%22Verweij%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22M%20C%20de%22%2C%22lastName%22%3A%22Bruijne%22%7D%5D%2C%22abstractNote%22%3A%22%22%2C%22reportNumber%22%3A%22%22%2C%22reportType%22%3A%22%22%2C%22institution%22%3A%22%22%2C%22date%22%3A%222017%22%2C%22language%22%3A%22nl%22%2C%22url%22%3A%22http%3A%5C%2F%5C%2Fwww.onderzoekpatientveiligheid.nl%22%2C%22collections%22%3A%5B%224EUQP96T%22%5D%2C%22dateModified%22%3A%222020-05-29T20%3A35%3A35Z%22%7D%7D%2C%7B%22key%22%3A%22ZNE4MJUH%22%2C%22library%22%3A%7B%22id%22%3A6637697%7D%2C%22meta%22%3A%7B%22parsedDate%22%3A%222019%22%2C%22numChildren%22%3A1%7D%2C%22bib%22%3A%22%3Cdiv%20class%3D%5C%22csl-bib-body%5C%22%20style%3D%5C%22line-height%3A%202%3B%20padding-left%3A%202em%3B%20text-indent%3A-2em%3B%5C%22%3E%5Cn%20%20%3Cdiv%20class%3D%5C%22csl-entry%5C%22%3E%3Ci%3EMANUAL%20ON%20BORDERLINE%20AND%20CLASSIFICATION%20IN%20THE%20COMMUNITY%20REGULATORY%20FRAMEWORK%20FOR%20MEDICAL%20DEVICES%3C%5C%2Fi%3E.%202019.%3C%5C%2Fdiv%3E%5Cn%3C%5C%2Fdiv%3E%22%2C%22data%22%3A%7B%22itemType%22%3A%22document%22%2C%22title%22%3A%22MANUAL%20ON%20BORDERLINE%20AND%20CLASSIFICATION%20IN%20THE%20COMMUNITY%20REGULATORY%20FRAMEWORK%20FOR%20MEDICAL%20DEVICES%22%2C%22creators%22%3A%5B%5D%2C%22abstractNote%22%3A%22%22%2C%22date%22%3A%225%5C%2F2019%22%2C%22language%22%3A%22en%22%2C%22url%22%3A%22%22%2C%22collections%22%3A%5B%224EUQP96T%22%5D%2C%22dateModified%22%3A%222020-05-29T20%3A21%3A05Z%22%7D%7D%2C%7B%22key%22%3A%22QZ92BH4G%22%2C%22library%22%3A%7B%22id%22%3A6637697%7D%2C%22meta%22%3A%7B%22parsedDate%22%3A%222017%22%2C%22numChildren%22%3A1%7D%2C%22bib%22%3A%22%3Cdiv%20class%3D%5C%22csl-bib-body%5C%22%20style%3D%5C%22line-height%3A%202%3B%20padding-left%3A%202em%3B%20text-indent%3A-2em%3B%5C%22%3E%5Cn%20%20%3Cdiv%20class%3D%5C%22csl-entry%5C%22%3E%3Ci%3EMANUAL%20ON%20BORDERLINE%20AND%20CLASSIFICATION%20IN%20THE%20COMMUNITY%26%23xA0%3B%20REGULATORY%20FRAMEWORK%20FOR%20MEDICAL%20DEVICES%3C%5C%2Fi%3E.%20EUR%2C%202017.%3C%5C%2Fdiv%3E%5Cn%3C%5C%2Fdiv%3E%22%2C%22data%22%3A%7B%22itemType%22%3A%22document%22%2C%22title%22%3A%22MANUAL%20ON%20BORDERLINE%20AND%20CLASSIFICATION%20IN%20THE%20COMMUNITY%20%20REGULATORY%20FRAMEWORK%20FOR%20MEDICAL%20DEVICES%22%2C%22creators%22%3A%5B%5D%2C%22abstractNote%22%3A%22%22%2C%22date%22%3A%2212-2017%22%2C%22language%22%3A%22en%22%2C%22url%22%3A%22%22%2C%22collections%22%3A%5B%224EUQP96T%22%5D%2C%22dateModified%22%3A%222020-05-29T20%3A19%3A06Z%22%7D%7D%2C%7B%22key%22%3A%22SR4PIVZF%22%2C%22library%22%3A%7B%22id%22%3A6637697%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22Schotanus%20et%20al.%22%2C%22parsedDate%22%3A%222018%22%2C%22numChildren%22%3A1%7D%2C%22bib%22%3A%22%3Cdiv%20class%3D%5C%22csl-bib-body%5C%22%20style%3D%5C%22line-height%3A%202%3B%20padding-left%3A%202em%3B%20text-indent%3A-2em%3B%5C%22%3E%5Cn%20%20%3Cdiv%20class%3D%5C%22csl-entry%5C%22%3ESchotanus%2C%20Fredo%2C%20et%20al.%20%3Ci%3EHandreiking%20Inkoop%20Hulpmiddelen.%20Geactualiseerde%20handreiking%20met%20afwegingen%2C%20uitdagingen%20en%20mogelijkheden%20voor%20gemeenten%20bij%20inkoop%20van%20Wmo-hulpmiddelen.%3C%5C%2Fi%3E%20VNG%2C%202018%2C%20%3Ca%20href%3D%27https%3A%5C%2F%5C%2Fvng.nl%5C%2Fpublicaties%5C%2Fhandreiking-inkoop-hulpmiddelen-0%27%3Ehttps%3A%5C%2F%5C%2Fvng.nl%5C%2Fpublicaties%5C%2Fhandreiking-inkoop-hulpmiddelen-0%3C%5C%2Fa%3E.%3C%5C%2Fdiv%3E%5Cn%3C%5C%2Fdiv%3E%22%2C%22data%22%3A%7B%22itemType%22%3A%22document%22%2C%22title%22%3A%22Handreiking%20Inkoop%20Hulpmiddelen.%20Geactualiseerde%20handreiking%20met%20afwegingen%2C%20uitdagingen%20en%20mogelijkheden%20voor%20gemeenten%20bij%20inkoop%20van%20Wmo-hulpmiddelen.%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Fredo%22%2C%22lastName%22%3A%22Schotanus%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Rick%22%2C%22lastName%22%3A%22Tuinman%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Jaap%22%2C%22lastName%22%3A%22Meijer%22%7D%5D%2C%22abstractNote%22%3A%22%22%2C%22date%22%3A%222018%22%2C%22language%22%3A%22nl%22%2C%22url%22%3A%22https%3A%5C%2F%5C%2Fvng.nl%5C%2Fpublicaties%5C%2Fhandreiking-inkoop-hulpmiddelen-0%22%2C%22collections%22%3A%5B%224EUQP96T%22%5D%2C%22dateModified%22%3A%222020-05-29T20%3A12%3A14Z%22%7D%7D%2C%7B%22key%22%3A%22A557M62H%22%2C%22library%22%3A%7B%22id%22%3A6637697%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22Peters%20et%20al.%22%2C%22parsedDate%22%3A%222014%22%2C%22numChildren%22%3A1%7D%2C%22bib%22%3A%22%3Cdiv%20class%3D%5C%22csl-bib-body%5C%22%20style%3D%5C%22line-height%3A%202%3B%20padding-left%3A%202em%3B%20text-indent%3A-2em%3B%5C%22%3E%5Cn%20%20%3Cdiv%20class%3D%5C%22csl-entry%5C%22%3EPeters%2C%20Chiel%2C%20et%20al.%20%3Ci%3EHandreiking%20Inkoop%20Hulpmiddelen.%20Afwegingen%2C%20uitdagingen%20en%20mogelijkheden%20voor%20gemeenten%20bij%20de%20inkoop%20van%20Wmo-hulpmiddelen.%3C%5C%2Fi%3E%20VNG%2C%200ktober%202014.%3C%5C%2Fdiv%3E%5Cn%3C%5C%2Fdiv%3E%22%2C%22data%22%3A%7B%22itemType%22%3A%22document%22%2C%22title%22%3A%22Handreiking%20Inkoop%20Hulpmiddelen.%20Afwegingen%2C%20uitdagingen%20en%20mogelijkheden%20voor%20gemeenten%20bij%20de%20inkoop%20van%20Wmo-hulpmiddelen.%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Chiel%22%2C%22lastName%22%3A%22Peters%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Fredo%22%2C%22lastName%22%3A%22Schotanus%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Lydia%22%2C%22lastName%22%3A%22Vunderink%22%7D%5D%2C%22abstractNote%22%3A%22%22%2C%22date%22%3A%220ktober%202014%22%2C%22language%22%3A%22nl-NL%22%2C%22url%22%3A%22%22%2C%22collections%22%3A%5B%224EUQP96T%22%2C%22DD8I76K6%22%5D%2C%22dateModified%22%3A%222020-05-29T20%3A04%3A22Z%22%7D%7D%2C%7B%22key%22%3A%22ZTCTTN83%22%2C%22library%22%3A%7B%22id%22%3A6637697%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22Ha%20et%20al.%22%2C%22parsedDate%22%3A%222000-10%22%2C%22numChildren%22%3A1%7D%2C%22bib%22%3A%22%3Cdiv%20class%3D%5C%22csl-bib-body%5C%22%20style%3D%5C%22line-height%3A%202%3B%20padding-left%3A%202em%3B%20text-indent%3A-2em%3B%5C%22%3E%5Cn%20%20%3Cdiv%20class%3D%5C%22csl-entry%5C%22%3EHa%2C%20DongRan%2C%20et%20al.%20%26%23x201C%3BEvaluation%20of%20Wheelchair%20Back%20Support%20Crashworthiness%3A%20Combination%20Wheelchair%20Back%20Support%20Surfaces%20and%20Attachment%20Hardware.%26%23x201D%3B%20%3Ci%3EJournal%20of%20Rehabilitation%20Research%3C%5C%2Fi%3E%2C%20vol.%2036%2C%20no.%205%2C%20Oct.%202000%2C%20pp.%20555%26%23x2013%3B63%2C%20%3Ca%20href%3D%27https%3A%5C%2F%5C%2Fpubmed.ncbi.nlm.nih.gov%5C%2F12135653%5C%2F%27%3Ehttps%3A%5C%2F%5C%2Fpubmed.ncbi.nlm.nih.gov%5C%2F12135653%5C%2F%3C%5C%2Fa%3E.%3C%5C%2Fdiv%3E%5Cn%3C%5C%2Fdiv%3E%22%2C%22data%22%3A%7B%22itemType%22%3A%22journalArticle%22%2C%22title%22%3A%22Evaluation%20of%20wheelchair%20back%20support%20crashworthiness%3A%20combination%20wheelchair%20back%20support%20surfaces%20and%20attachment%20hardware%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22DongRan%22%2C%22lastName%22%3A%22Ha%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Gina%22%2C%22lastName%22%3A%22Bertocci%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Ernest%22%2C%22lastName%22%3A%22Deemer%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Linda%20van%22%2C%22lastName%22%3A%22Roosmalen%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Patricia%22%2C%22lastName%22%3A%22Karg%22%7D%5D%2C%22abstractNote%22%3A%22%22%2C%22date%22%3A%22september%5C%2Foctober%202000%22%2C%22language%22%3A%22en%22%2C%22DOI%22%3A%22%22%2C%22ISSN%22%3A%22%22%2C%22url%22%3A%22https%3A%5C%2F%5C%2Fpubmed.ncbi.nlm.nih.gov%5C%2F12135653%5C%2F%22%2C%22collections%22%3A%5B%224EUQP96T%22%5D%2C%22dateModified%22%3A%222020-05-29T19%3A56%3A38Z%22%7D%7D%2C%7B%22key%22%3A%2258XFKV69%22%2C%22library%22%3A%7B%22id%22%3A6637697%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22Plomp%22%2C%22numChildren%22%3A1%7D%2C%22bib%22%3A%22%3Cdiv%20class%3D%5C%22csl-bib-body%5C%22%20style%3D%5C%22line-height%3A%202%3B%20padding-left%3A%202em%3B%20text-indent%3A-2em%3B%5C%22%3E%5Cn%20%20%3Cdiv%20class%3D%5C%22csl-entry%5C%22%3EPlomp%2C%20Mr.%20M.%20J.%20%26%23x201C%3BKroniek%20concentratie%20controle.%26%23x201D%3B%20%3Ci%3EMarkt%20en%20Mededinging%3C%5C%2Fi%3E.%3C%5C%2Fdiv%3E%5Cn%3C%5C%2Fdiv%3E%22%2C%22data%22%3A%7B%22itemType%22%3A%22magazineArticle%22%2C%22title%22%3A%22Kroniek%20concentratie%20controle%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Mr.%20M.J.%22%2C%22lastName%22%3A%22Plomp%22%7D%5D%2C%22abstractNote%22%3A%22%22%2C%22date%22%3A%22%22%2C%22language%22%3A%22nl-NL%22%2C%22ISSN%22%3A%22%22%2C%22url%22%3A%22%22%2C%22collections%22%3A%5B%224EUQP96T%22%5D%2C%22dateModified%22%3A%222020-05-29T19%3A32%3A58Z%22%7D%7D%2C%7B%22key%22%3A%222ZEXSUHR%22%2C%22library%22%3A%7B%22id%22%3A6637697%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22Heerdink%22%2C%22parsedDate%22%3A%222011-07-07%22%2C%22numChildren%22%3A1%7D%2C%22bib%22%3A%22%3Cdiv%20class%3D%5C%22csl-bib-body%5C%22%20style%3D%5C%22line-height%3A%202%3B%20padding-left%3A%202em%3B%20text-indent%3A-2em%3B%5C%22%3E%5Cn%20%20%3Cdiv%20class%3D%5C%22csl-entry%5C%22%3EHeerdink%2C%20M.%20E.%20S.%20%3Ci%3EEen%20Goede%20Zithouding%2C%20Dat%20Loont%21%20Een%20Onderzoek%20Naar%20de%20Invloed%20van%20Een%20Anatomisch%20Verantwoorde%20En%20Stabiele%20Zitondersteuning%20Op%20de%20Kostenbesparingen%20in%20de%20Zorg.%3C%5C%2Fi%3E%207%20July%202011%2C%20%3Ca%20href%3D%27https%3A%5C%2F%5C%2Fessay.utwente.nl%5C%2F62933%5C%2F%27%3Ehttps%3A%5C%2F%5C%2Fessay.utwente.nl%5C%2F62933%5C%2F%3C%5C%2Fa%3E.%3C%5C%2Fdiv%3E%5Cn%3C%5C%2Fdiv%3E%22%2C%22data%22%3A%7B%22itemType%22%3A%22webpage%22%2C%22title%22%3A%22Een%20goede%20zithouding%2C%20dat%20loont%21%20Een%20onderzoek%20naar%20de%20invloed%20van%20een%20anatomisch%20verantwoorde%20en%20stabiele%20zitondersteuning%20op%20de%20kostenbesparingen%20in%20de%20zorg.%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22M.%20E.%20S.%22%2C%22lastName%22%3A%22Heerdink%22%7D%5D%2C%22abstractNote%22%3A%22In%20een%20periode%20van%20%5Cu00b1%2010%20jaar%20is%20onderzoek%20gedaan%20naar%20zitproblemen%2C%20met%20als%20doel%20de%20zitkwaliteit%20te%20objectiveren%20en%20te%20verbeteren.%20Een%20van%20de%20resultaten%20van%20dit%20onderzoek%20was%20het%20SMS-zitadvies%2C%20een%20meetinstrument%20dat%20ingezet%20kan%20worden%20bij%20de%20selectie%20van%20een%20meest%20adequate%20zit-%20en%20rugondersteuning%20voor%20een%20bepaald%20persoon.%20Vanuit%20het%20SMS%20zitadvies%20is%20de%20term%20anatomisch%20verantwoord%20en%20stabiel%20zitten%20ontstaan.%20Uit%20ervaring%20blijkt%20dat%20een%20anatomisch%20verantwoorde%20en%20stabiele%20%28AVeS%29%20zitondersteuning%20een%20erg%20positieve%20invloed%20heeft%20op%20de%20levenskwaliteit%20van%20permanent%20langdurige%20rolstoelgebruikers.%20Zorgkantoren%20%5Cu2013%20financiers%20van%20de%20zitvoorzieningen%20%5Cu2013%20zijn%20echter%20niet%20altijd%20overtuigd%20van%20het%20anatomisch%20verantwoord%20en%20stabiel%20zitten.%20Objectief%20onderzoek%20naar%20de%20invloed%20van%20een%20anatomisch%20verantwoorde%20en%20stabiele%20zitondersteuning%20op%20de%20kosten%20in%20de%20zorg%20zou%20hier%20meer%20inzicht%20kunnen%20bieden.%20De%20onderzoeksvraag%20die%20centraal%20staat%20in%20deze%20scriptie%20is%20dan%20ook%3A%5CnWat%20is%20de%20invloed%20van%20een%20toegepaste%20anatomisch%20verantwoorde%20en%20stabiele%20zitondersteuning%20op%20de%20kosten%20in%20de%20zorg%3F%22%2C%22date%22%3A%222011-07-07%22%2C%22url%22%3A%22https%3A%5C%2F%5C%2Fessay.utwente.nl%5C%2F62933%5C%2F%22%2C%22language%22%3A%22en%22%2C%22collections%22%3A%5B%224EUQP96T%22%5D%2C%22dateModified%22%3A%222020-05-29T09%3A39%3A09Z%22%7D%7D%2C%7B%22key%22%3A%22XXIR5T2D%22%2C%22library%22%3A%7B%22id%22%3A6637697%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22Akerlof%20et%20al.%22%2C%22parsedDate%22%3A%222017%22%2C%22numChildren%22%3A0%7D%2C%22bib%22%3A%22%3Cdiv%20class%3D%5C%22csl-bib-body%5C%22%20style%3D%5C%22line-height%3A%202%3B%20padding-left%3A%202em%3B%20text-indent%3A-2em%3B%5C%22%3E%5Cn%20%20%3Cdiv%20class%3D%5C%22csl-entry%5C%22%3EAkerlof%2C%20George%20A.%2C%20et%20al.%20%3Ci%3EDe%20economie%20van%20list%20en%20bedrog%3C%5C%2Fi%3E.%202017.%3C%5C%2Fdiv%3E%5Cn%3C%5C%2Fdiv%3E%22%2C%22data%22%3A%7B%22itemType%22%3A%22book%22%2C%22title%22%3A%22De%20economie%20van%20list%20en%20bedrog%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22George%20A%22%2C%22lastName%22%3A%22Akerlof%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Robert%20J%22%2C%22lastName%22%3A%22Shiller%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Joost%22%2C%22lastName%22%3A%22Mulder%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22George%20A%22%2C%22lastName%22%3A%22Akerlof%22%7D%5D%2C%22abstractNote%22%3A%22%22%2C%22date%22%3A%222017%22%2C%22language%22%3A%22Dutch%22%2C%22ISBN%22%3A%22978-94-6298-353-3%22%2C%22url%22%3A%22%22%2C%22collections%22%3A%5B%224EUQP96T%22%5D%2C%22dateModified%22%3A%222020-05-29T09%3A18%3A45Z%22%7D%7D%2C%7B%22key%22%3A%22V6RV3QPD%22%2C%22library%22%3A%7B%22id%22%3A6637697%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22Kok%20et%20al.%22%2C%22parsedDate%22%3A%222008%22%2C%22numChildren%22%3A1%7D%2C%22bib%22%3A%22%3Cdiv%20class%3D%5C%22csl-bib-body%5C%22%20style%3D%5C%22line-height%3A%202%3B%20padding-left%3A%202em%3B%20text-indent%3A-2em%3B%5C%22%3E%5Cn%20%20%3Cdiv%20class%3D%5C%22csl-entry%5C%22%3EKok%2C%20L.%2C%20et%20al.%20%3Ci%3EKosten%20en%20baten%20van%20revalidatie%3C%5C%2Fi%3E.%20SEO%2C%202008.%3C%5C%2Fdiv%3E%5Cn%3C%5C%2Fdiv%3E%22%2C%22data%22%3A%7B%22itemType%22%3A%22book%22%2C%22title%22%3A%22Kosten%20en%20baten%20van%20revalidatie%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22L%22%2C%22lastName%22%3A%22Kok%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22A%22%2C%22lastName%22%3A%22Houkes%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22N%22%2C%22lastName%22%3A%22Niessen%22%7D%5D%2C%22abstractNote%22%3A%22%22%2C%22date%22%3A%222008%22%2C%22language%22%3A%22No%20Linguistic%20Content%22%2C%22ISBN%22%3A%22978-90-6733-469-3%22%2C%22url%22%3A%22%22%2C%22collections%22%3A%5B%224EUQP96T%22%5D%2C%22dateModified%22%3A%222020-05-28T21%3A17%3A28Z%22%7D%7D%2C%7B%22key%22%3A%227XFH95YB%22%2C%22library%22%3A%7B%22id%22%3A6637697%7D%2C%22meta%22%3A%7B%22numChildren%22%3A1%7D%2C%22bib%22%3A%22%3Cdiv%20class%3D%5C%22csl-bib-body%5C%22%20style%3D%5C%22line-height%3A%202%3B%20padding-left%3A%202em%3B%20text-indent%3A-2em%3B%5C%22%3E%5Cn%20%20%3Cdiv%20class%3D%5C%22csl-entry%5C%22%3E%3Ci%3ERERC_WTS%3A%20Research%20Tasks%2C%20SP-1b%20In-Depth%20Investigation%20Accidents%20in%20Motor%20Vehicles%3C%5C%2Fi%3E.%20%3Ca%20href%3D%27http%3A%5C%2F%5C%2Fwww.rercwts.org%5C%2FRERC_WTS_Research%5C%2FRERC1_WTS_Research%5C%2FRERC_WTS_Res_SP%5C%2FRERC_WTS_Res_SP1b%5C%2FRERC_WTS_res_sp1b.html%27%3Ehttp%3A%5C%2F%5C%2Fwww.rercwts.org%5C%2FRERC_WTS_Research%5C%2FRERC1_WTS_Research%5C%2FRERC_WTS_Res_SP%5C%2FRERC_WTS_Res_SP1b%5C%2FRERC_WTS_res_sp1b.html%3C%5C%2Fa%3E.%20Accessed%2028%20May%202020.%3C%5C%2Fdiv%3E%5Cn%3C%5C%2Fdiv%3E%22%2C%22data%22%3A%7B%22itemType%22%3A%22webpage%22%2C%22title%22%3A%22RERC_WTS%3A%20Research%20Tasks%2C%20SP-1b%20In-Depth%20Investigation%20Accidents%20in%20Motor%20Vehicles%22%2C%22creators%22%3A%5B%5D%2C%22abstractNote%22%3A%22%22%2C%22date%22%3A%22%22%2C%22url%22%3A%22http%3A%5C%2F%5C%2Fwww.rercwts.org%5C%2FRERC_WTS_Research%5C%2FRERC1_WTS_Research%5C%2FRERC_WTS_Res_SP%5C%2FRERC_WTS_Res_SP1b%5C%2FRERC_WTS_res_sp1b.html%22%2C%22language%22%3A%22%22%2C%22collections%22%3A%5B%224EUQP96T%22%2C%22DD8I76K6%22%5D%2C%22dateModified%22%3A%222020-05-28T14%3A47%3A55Z%22%7D%7D%2C%7B%22key%22%3A%22BR4MCUK3%22%2C%22library%22%3A%7B%22id%22%3A6637697%7D%2C%22meta%22%3A%7B%22numChildren%22%3A1%7D%2C%22bib%22%3A%22%3Cdiv%20class%3D%5C%22csl-bib-body%5C%22%20style%3D%5C%22line-height%3A%202%3B%20padding-left%3A%202em%3B%20text-indent%3A-2em%3B%5C%22%3E%5Cn%20%20%3Cdiv%20class%3D%5C%22csl-entry%5C%22%3E%3Ci%3EWheelchairs%20-%20WC%20Transportation%20Safety%3C%5C%2Fi%3E.%20%3Ca%20href%3D%27http%3A%5C%2F%5C%2Fwc-transportation-safety.umtri.umich.edu%5C%2Fcrash-tested-product-lists%5C%2Fwheelchairs%27%3Ehttp%3A%5C%2F%5C%2Fwc-transportation-safety.umtri.umich.edu%5C%2Fcrash-tested-product-lists%5C%2Fwheelchairs%3C%5C%2Fa%3E.%20Accessed%2028%20May%202020.%3C%5C%2Fdiv%3E%5Cn%3C%5C%2Fdiv%3E%22%2C%22data%22%3A%7B%22itemType%22%3A%22webpage%22%2C%22title%22%3A%22Wheelchairs%20-%20WC%20Transportation%20Safety%22%2C%22creators%22%3A%5B%5D%2C%22abstractNote%22%3A%22%22%2C%22date%22%3A%22%22%2C%22url%22%3A%22http%3A%5C%2F%5C%2Fwc-transportation-safety.umtri.umich.edu%5C%2Fcrash-tested-product-lists%5C%2Fwheelchairs%22%2C%22language%22%3A%22%22%2C%22collections%22%3A%5B%224EUQP96T%22%5D%2C%22dateModified%22%3A%222020-05-28T14%3A34%3A01Z%22%7D%7D%2C%7B%22key%22%3A%22Y6Y5ZEGP%22%2C%22library%22%3A%7B%22id%22%3A6637697%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22Willemsen%20et%20al.%22%2C%22parsedDate%22%3A%222019-08-01%22%2C%22numChildren%22%3A2%7D%2C%22bib%22%3A%22%3Cdiv%20class%3D%5C%22csl-bib-body%5C%22%20style%3D%5C%22line-height%3A%202%3B%20padding-left%3A%202em%3B%20text-indent%3A-2em%3B%5C%22%3E%5Cn%20%20%3Cdiv%20class%3D%5C%22csl-entry%5C%22%3EWillemsen%2C%20Koen%2C%20et%20al.%20%26%23x201C%3BChallenges%20in%20the%20Design%20and%20Regulatory%20Approval%20of%203D-Printed%20Surgical%20Implants%3A%20A%20Two-Case%20Series.%26%23x201D%3B%20%3Ci%3EThe%20Lancet%20Digital%20Health%3C%5C%2Fi%3E%2C%20vol.%201%2C%20no.%204%2C%20Aug.%202019%2C%20pp.%20e163%26%23x2013%3B71%2C%20%3Ca%20href%3D%27http%3A%5C%2F%5C%2Fdoi.org%5C%2F10.1016%5C%2FS2589-7500%2819%2930067-6%27%3Ehttp%3A%5C%2F%5C%2Fdoi.org%5C%2F10.1016%5C%2FS2589-7500%2819%2930067-6%3C%5C%2Fa%3E.%3C%5C%2Fdiv%3E%5Cn%3C%5C%2Fdiv%3E%22%2C%22data%22%3A%7B%22itemType%22%3A%22journalArticle%22%2C%22title%22%3A%22Challenges%20in%20the%20design%20and%20regulatory%20approval%20of%203D-printed%20surgical%20implants%3A%20a%20two-case%20series%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Koen%22%2C%22lastName%22%3A%22Willemsen%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Razmara%22%2C%22lastName%22%3A%22Nizak%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Herke%20Jan%22%2C%22lastName%22%3A%22Noordmans%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Ren%5Cu00e9%20M.%22%2C%22lastName%22%3A%22Castelein%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Harrie%22%2C%22lastName%22%3A%22Weinans%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Moyo%20C.%22%2C%22lastName%22%3A%22Kruyt%22%7D%5D%2C%22abstractNote%22%3A%22%3Ch2%3ESummary%3C%5C%2Fh2%3E%3Ch3%3EBackground%3C%5C%2Fh3%3E%3Cp%3EAdditive%20manufacturing%20or%20three-dimensional%20%283D%29%20printing%20of%20metal%20implants%20can%20provide%20novel%20solutions%20for%20difficult-to-treat%20conditions%2C%20yet%20legislation%20concerning%20patient-specific%20implants%20complicates%20the%20implementation%20of%20these%20techniques%20in%20daily%20practice.%20In%20this%20Article%2C%20we%20share%20our%20acquired%20knowledge%20of%20the%20logistical%20and%20legal%20challenges%20associated%20with%20the%20use%20of%20patient-specific%203D-printed%20implants%20to%20treat%20spinal%20instabilities.%3C%5C%2Fp%3E%3Ch3%3EMethods%3C%5C%2Fh3%3E%3Cp%3ETwo%20patients%20with%20semiurgent%20cases%20of%20spinal%20instability%20presented%20to%20our%20hospital%20in%20the%20Netherlands.%20In%20case%201%2C%20severe%20kyphotic%20deformity%20of%20the%20thoracic%20spine%20due%20to%20neurofibromatosis%20type%201%20had%20led%20to%20incomplete%20paralysis%2C%20and%20a%20strong%20metallic%20strut%20extending%20from%20C6%20to%20T11%20was%20deemed%20necessary%20to%20provide%20long-term%20anterior%20support.%20In%20case%202%2C%20the%20patient%20presented%20with%20progressive%20paralysis%20caused%20by%20cervicothoracic%20dissociation%20due%20to%20vanishing%20bone%20disease.%20As%20the%20C5%5Cu2013T1%20vertebral%20bodies%20had%20mostly%20vanished%2C%20an%20implant%20spanning%20the%20anterior%20spine%20from%20C4%20to%20T2%20was%20required.%20Because%20of%20the%20complex%20and%20challenging%20nature%20of%20both%20cases%2C%20conventional%20approaches%20were%20deemed%20inadequate%3B%20instead%2C%20patient-specific%20implants%20were%20designed%20with%20use%20of%20CT%20scans%20and%20computer-aided%20design%20software%2C%20and%203D%20printed%20in%20titanium%20with%20direct%20metal%20printing.%20For%20each%20implant%2C%20to%20ensure%20patient%20safety%2C%20a%20comprehensive%20technical%20file%20%28describing%20the%20clinical%20substantiation%2C%20technical%20and%20design%20considerations%2C%20risk%20analysis%2C%20manufacturing%20process%2C%20and%20labelling%29%20was%20produced%20in%20collaboration%20with%20a%20university%20department%20certified%20for%20the%20development%20and%20manufacturing%20of%20medical%20devices.%20Because%20the%20implants%20were%20categorised%20as%20custom-made%20or%20personalised%20devices%20under%20the%20EU%20Medical%20Device%20Regulation%2C%20the%20usual%20procedures%20for%20review%20and%20approval%20of%20medical%20devices%20by%20a%20notified%20body%20were%20not%20required.%20Finite-element%20analyses%2C%20compression%20strength%20tests%2C%20and%20cadaveric%20experiments%20were%20also%20done%20to%20ensure%20the%20devices%20were%20safe%20to%20use.%3C%5C%2Fp%3E%3Ch3%3EFindings%3C%5C%2Fh3%3E%3Cp%3EThe%20planning%2C%20design%2C%20production%2C%20and%20insertion%20of%20the%203D-printed%20personalised%20implant%20took%20around%206%20months%20in%20the%20first%20patient%2C%20but%2C%20given%20the%20experience%20from%20the%20first%20case%2C%20only%20took%20around%206%20weeks%20in%20the%20second%20patient.%20In%20both%20patients%2C%20the%20surgeries%20went%20as%20planned%20and%20good%20positioning%20of%20each%20implant%20was%20confirmed.%20Both%20patients%20were%20discharged%20home%20within%201%20week%20after%20the%20surgery.%20In%20the%20first%20patient%2C%20a%20fatigue%20fracture%20occured%20in%20one%20of%20the%20conventional%20posterior%20fusion%20rods%20after%2010%20months%2C%20which%20we%20repaired%2C%20without%20any%20deformation%20of%20the%20spine%20or%20signs%20of%20failure%20of%20the%20personalised%20implant%20observed.%20No%20other%20adverse%20events%20occurred%20up%20to%2025%20months%20of%20follow-up%20in%20case%201%20and%206%20months%20of%20follow-up%20in%20case%202.%3C%5C%2Fp%3E%3Ch3%3EInterpretation%3C%5C%2Fh3%3E%3Cp%3EPatient-specific%20treatment%20approaches%20incorporating%203D-printed%20implants%20can%20be%20helpful%20in%20carefully%20selected%20cases%20when%20conventional%20methods%20are%20not%20an%20option.%20Comprehensive%20and%20efficient%20interactions%20between%20medical%20engineers%20and%20physicians%20are%20essential%20to%20establish%20well%20designed%20frameworks%20to%20navigate%20the%20logistical%20and%20regulatory%20aspects%20of%20technology%20development%20to%20ensure%20the%20safety%20and%20legal%20validity%20of%20patient-specific%20treatments.%20The%20framework%20described%20here%20could%20encourage%20physicians%20to%20treat%20%28once%20untreatable%29%20patients%20with%20novel%20personalised%20techniques.%3C%5C%2Fp%3E%3Ch3%3EFunding%3C%5C%2Fh3%3E%3Cp%3EInterreg%20VA%20Flanders%5Cu2014The%20Netherlands%20programme%2C%20Applied%20and%20Engineering%20Sciences%20research%20programme%2C%20the%20Netherlands%20Organisation%20for%20Scientific%20Research%2C%20and%20the%20Dutch%20Arthritis%20Foundation%3C%5C%2Fp%3E%3Ch3%3EVideo%20Abstract%3C%5C%2Fh3%3E%22%2C%22date%22%3A%222019%5C%2F08%5C%2F01%22%2C%22language%22%3A%22English%22%2C%22DOI%22%3A%2210.1016%5C%2FS2589-7500%2819%2930067-6%22%2C%22ISSN%22%3A%222589-7500%22%2C%22url%22%3A%22https%3A%5C%2F%5C%2Fwww.thelancet.com%5C%2Fjournals%5C%2Flandig%5C%2Farticle%5C%2FPIIS2589-7500%2819%2930067-6%5C%2Fabstract%22%2C%22collections%22%3A%5B%224EUQP96T%22%5D%2C%22dateModified%22%3A%222020-05-28T11%3A08%3A30Z%22%7D%7D%2C%7B%22key%22%3A%22287P977H%22%2C%22library%22%3A%7B%22id%22%3A6637697%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22Zackowitz%20and%20Vredenburgh%22%2C%22parsedDate%22%3A%222007-10-01%22%2C%22numChildren%22%3A0%7D%2C%22bib%22%3A%22%3Cdiv%20class%3D%5C%22csl-bib-body%5C%22%20style%3D%5C%22line-height%3A%202%3B%20padding-left%3A%202em%3B%20text-indent%3A-2em%3B%5C%22%3E%5Cn%20%20%3Cdiv%20class%3D%5C%22csl-entry%5C%22%3EZackowitz%2C%20Ilene%20B.%2C%20and%20Alison%20G.%20Vredenburgh.%20%26%23x201C%3BWhen%20Communication%20Failure%20Contributes%20to%20an%20Injury%3A%20A%20Case%20Study%20of%20Para-Transportation%20for%20Wheelchair%20Users.%26%23x201D%3B%20%3Ci%3EProceedings%20of%20the%20Human%20Factors%20and%20Ergonomics%20Society%20Annual%20Meeting%3C%5C%2Fi%3E%2C%20vol.%2051%2C%20no.%209%2C%20Oct.%202007%2C%20pp.%20559%26%23x2013%3B63%2C%20%3Ca%20href%3D%27http%3A%5C%2F%5C%2Fdoi.org%5C%2F10.1177%5C%2F154193120705100902%27%3Ehttp%3A%5C%2F%5C%2Fdoi.org%5C%2F10.1177%5C%2F154193120705100902%3C%5C%2Fa%3E.%3C%5C%2Fdiv%3E%5Cn%3C%5C%2Fdiv%3E%22%2C%22data%22%3A%7B%22itemType%22%3A%22journalArticle%22%2C%22title%22%3A%22When%20Communication%20Failure%20Contributes%20to%20an%20Injury%3A%20A%20Case%20Study%20of%20Para-Transportation%20for%20Wheelchair%20Users%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Ilene%20B.%22%2C%22lastName%22%3A%22Zackowitz%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Alison%20G.%22%2C%22lastName%22%3A%22Vredenburgh%22%7D%5D%2C%22abstractNote%22%3A%22Our%20firm%20was%20retained%20to%20investigate%20an%20injury%20sustained%20by%20an%20elderly%20woman%20who%20was%20confined%20to%20a%20wheelchair%20at%20the%20time%20of%20the%20incident.%20The%20woman%20was%20utilizing%20a%20public%20para-transportation%20service%20for%20people%20with%20disabilities%20when%20the%20van%20she%20was%20riding%20stopped%20short.%20As%20a%20result%2C%20she%20slid%20out%20of%20her%20wheelchair%20and%20suffered%20a%20compound%20fracture%20of%20the%20leg.%20This%20case%20went%20to%20trial%20with%20the%20seatbelt%20manufacturer%20and%20transportation%20entity%20as%20defendants.%20Looking%20beyond%20the%20obvious%20issues%20of%20seatbelt%20failure%20and%20driver%20training%2C%20this%20paper%20will%20examine%20communication%20as%20a%20necessary%20part%20of%20the%20safety%20system.%20Communication%20involves%20the%20sharing%20of%20information%20in%20a%20complex%20system%20where%20users%20are%20not%20domain%20experts.%20In%20this%20case%2C%20communication%20as%20part%20of%20a%20public%20para-transportation%20safety%20system%20is%20evaluated.%22%2C%22date%22%3A%22October%201%2C%202007%22%2C%22language%22%3A%22en%22%2C%22DOI%22%3A%2210.1177%5C%2F154193120705100902%22%2C%22ISSN%22%3A%222169-5067%22%2C%22url%22%3A%22https%3A%5C%2F%5C%2Fdoi.org%5C%2F10.1177%5C%2F154193120705100902%22%2C%22collections%22%3A%5B%22DD8I76K6%22%5D%2C%22dateModified%22%3A%222020-05-27T23%3A03%3A09Z%22%7D%7D%2C%7B%22key%22%3A%22Q5EHJR5A%22%2C%22library%22%3A%7B%22id%22%3A6637697%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22Priest%22%2C%22parsedDate%22%3A%221988%22%2C%22numChildren%22%3A0%7D%2C%22bib%22%3A%22%3Cdiv%20class%3D%5C%22csl-bib-body%5C%22%20style%3D%5C%22line-height%3A%202%3B%20padding-left%3A%202em%3B%20text-indent%3A-2em%3B%5C%22%3E%5Cn%20%20%3Cdiv%20class%3D%5C%22csl-entry%5C%22%3EPriest%2C%20George%20L.%20%26%23x201C%3BStrict%20Products%20Liability%3A%20The%20Original%20Intent.%26%23x201D%3B%20%3Ci%3ECardozo%20Law%20Review%3C%5C%2Fi%3E%2C%20vol.%2010%2C%201989%201988%2C%20p.%202301%2C%20%3Ca%20href%3D%27https%3A%5C%2F%5C%2Fheinonline.org%5C%2FHOL%5C%2FPage%3Fhandle%3Dhein.journals%5C%2Fcdozo10%26id%3D2319%26div%3D%26collection%3D%27%3Ehttps%3A%5C%2F%5C%2Fheinonline.org%5C%2FHOL%5C%2FPage%3Fhandle%3Dhein.journals%5C%2Fcdozo10%26id%3D2319%26div%3D%26collection%3D%3C%5C%2Fa%3E.%3C%5C%2Fdiv%3E%5Cn%3C%5C%2Fdiv%3E%22%2C%22data%22%3A%7B%22itemType%22%3A%22journalArticle%22%2C%22title%22%3A%22Strict%20Products%20Liability%3A%20The%20Original%20Intent%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22George%20L.%22%2C%22lastName%22%3A%22Priest%22%7D%5D%2C%22abstractNote%22%3A%22%22%2C%22date%22%3A%221988-1989%22%2C%22language%22%3A%22%22%2C%22DOI%22%3A%22%22%2C%22ISSN%22%3A%22%22%2C%22url%22%3A%22https%3A%5C%2F%5C%2Fheinonline.org%5C%2FHOL%5C%2FPage%3Fhandle%3Dhein.journals%5C%2Fcdozo10%26id%3D2319%26div%3D%26collection%3D%22%2C%22collections%22%3A%5B%224EUQP96T%22%5D%2C%22dateModified%22%3A%222020-05-27T22%3A53%3A17Z%22%7D%7D%2C%7B%22key%22%3A%2293XCFR9K%22%2C%22library%22%3A%7B%22id%22%3A6637697%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22MSD%20et%20al.%22%2C%22parsedDate%22%3A%222007-12-31%22%2C%22numChildren%22%3A0%7D%2C%22bib%22%3A%22%3Cdiv%20class%3D%5C%22csl-bib-body%5C%22%20style%3D%5C%22line-height%3A%202%3B%20padding-left%3A%202em%3B%20text-indent%3A-2em%3B%5C%22%3E%5Cn%20%20%3Cdiv%20class%3D%5C%22csl-entry%5C%22%3EMSD%2C%20Peter%20J.%20Wolf%2C%20et%20al.%20%26%23x201C%3BWheelchair%20Tiedown%20and%20Occupant%20Restraint%20System%20Issues%20in%20the%20Real%20World%20and%20the%20Virtual%20World%3A%20Combining%20Qualitative%20and%20Quantitative%20Research%20Approaches.%26%23x201D%3B%20%3Ci%3EAssistive%20Technology%3C%5C%2Fi%3E%2C%20vol.%2019%2C%20no.%204%2C%20Dec.%202007%2C%20pp.%20188%26%23x2013%3B99%2C%20%3Ca%20href%3D%27http%3A%5C%2F%5C%2Fdoi.org%5C%2F10.1080%5C%2F10400435.2007.10131876%27%3Ehttp%3A%5C%2F%5C%2Fdoi.org%5C%2F10.1080%5C%2F10400435.2007.10131876%3C%5C%2Fa%3E.%3C%5C%2Fdiv%3E%5Cn%3C%5C%2Fdiv%3E%22%2C%22data%22%3A%7B%22itemType%22%3A%22journalArticle%22%2C%22title%22%3A%22Wheelchair%20Tiedown%20and%20Occupant%20Restraint%20System%20Issues%20in%20the%20Real%20World%20and%20the%20Virtual%20World%3A%20Combining%20Qualitative%20and%20Quantitative%20Research%20Approaches%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Peter%20J.%20Wolf%22%2C%22lastName%22%3A%22MSD%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Linda%20van%20Roosmalen%22%2C%22lastName%22%3A%22PhD%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Gina%20E.%20Bertocci%22%2C%22lastName%22%3A%22PhD%22%7D%5D%2C%22abstractNote%22%3A%22The%20Americans%20with%20Disabilities%20Act%20requires%20that%20transit%20providers%20accommodate%20passengers%20who%20use%20%5Cu201ccommon%20wheelchairs%5Cu201d%20when%20traveling%20in%20a%20motor%20vehicle.%20Wheelchair%20tiedown%20and%20occupant%20restraint%20systems%20are%20commonly%20used%20to%20secure%20wheelchairs%20and%20restrain%20occupants%20in%20fixed-route%20and%20demand%20route%20transit%20vehicles.%20Throughout%20the%2017%20years%20since%20the%20Americans%20with%20Disabilities%20Act%20has%20been%20in%20effect%2C%20transit%20providers%20have%20complained%20about%20the%20usability%20of%20wheelchair%20tiedown%20and%20occupant%20restraint%20systems%2C%20and%20improper%20securement%20has%20been%20linked%20to%20injuries%20among%20wheelchair%20users%20during%20%5Cu201cnonimpact%20incidents.%5Cu201d%20This%20research%20study%20explored%20the%20use%20of%20wheelchair%20tiedown%20and%20occupant%20restraint%20systems%20in%20actual%20practice%20and%20the%20potential%20risks%20of%20misuse%20to%20wheelchair-seated%20individuals.%20The%20qualitative%20research%20conducted%20in%20this%20study%20revealed%20that%20improper%20wheelchair%20securement%20%28i.e.%20using%20less%20than%20four%20tiedown%20straps%29%20can%20be%20fairly%20common%20practice%20in%20fixed-route%20transit.%20In%20addition%2C%20preliminary%20computer%20simulations%20show%20that%20improper%20wheelchair%20securement%20in%20emergency%20driving%20conditions%20may%20place%20wheelchair%20occupants%20at%20a%20greater%20risk%20of%20injury.%20It%20should%20be%20noted%2C%20however%2C%20that%20this%20is%20a%20pilot%20study%20and%20has%20its%20limitations.%20For%20example%2C%20qualitative%20data%20were%20gathered%20from%20one%20metropolitan%20area%20transit%20provider%20across%20a%20limited%20range%20of%20vehicle%20and%20wheelchair%20types.%20Additionally%2C%20the%20computer%20simulation%20model%20used%20in%20this%20study%20was%20originally%20validated%20for%20impact%20situations.%22%2C%22date%22%3A%22December%2031%2C%202007%22%2C%22language%22%3A%22%22%2C%22DOI%22%3A%2210.1080%5C%2F10400435.2007.10131876%22%2C%22ISSN%22%3A%221040-0435%22%2C%22url%22%3A%22https%3A%5C%2F%5C%2Fdoi.org%5C%2F10.1080%5C%2F10400435.2007.10131876%22%2C%22collections%22%3A%5B%224EUQP96T%22%5D%2C%22dateModified%22%3A%222020-05-27T22%3A09%3A00Z%22%7D%7D%2C%7B%22key%22%3A%22M4NU4MPV%22%2C%22library%22%3A%7B%22id%22%3A6637697%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22Peters%2C%20A.%22%2C%22parsedDate%22%3A%222019-01-01%22%2C%22numChildren%22%3A1%7D%2C%22bib%22%3A%22%3Cdiv%20class%3D%5C%22csl-bib-body%5C%22%20style%3D%5C%22line-height%3A%202%3B%20padding-left%3A%202em%3B%20text-indent%3A-2em%3B%5C%22%3E%5Cn%20%20%3Cdiv%20class%3D%5C%22csl-entry%5C%22%3EPeters%2C%20A.%20%3Ci%3ECode%20VVR%202019-2020%3C%5C%2Fi%3E.%20A.%20Peters%2C%201%20Jan.%202019%2C%20%3Ca%20href%3D%27http%3A%5C%2F%5C%2Fcodevvr.nl%27%3Ehttp%3A%5C%2F%5C%2Fcodevvr.nl%3C%5C%2Fa%3E.%3C%5C%2Fdiv%3E%5Cn%3C%5C%2Fdiv%3E%22%2C%22data%22%3A%7B%22itemType%22%3A%22document%22%2C%22title%22%3A%22Code%20VVR%202019-2020%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22%22%2C%22lastName%22%3A%22Peters%2C%20A.%22%7D%5D%2C%22abstractNote%22%3A%22%22%2C%22date%22%3A%221%20januari%202019%22%2C%22language%22%3A%22nl%22%2C%22url%22%3A%22http%3A%5C%2F%5C%2Fcodevvr.nl%22%2C%22collections%22%3A%5B%224EUQP96T%22%2C%22DD8I76K6%22%5D%2C%22dateModified%22%3A%222020-05-27T19%3A13%3A34Z%22%7D%7D%2C%7B%22key%22%3A%22V235NR99%22%2C%22library%22%3A%7B%22id%22%3A6637697%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22Kirby%20et%20al.%22%2C%22parsedDate%22%3A%221995-12-01%22%2C%22numChildren%22%3A0%7D%2C%22bib%22%3A%22%3Cdiv%20class%3D%5C%22csl-bib-body%5C%22%20style%3D%5C%22line-height%3A%202%3B%20padding-left%3A%202em%3B%20text-indent%3A-2em%3B%5C%22%3E%5Cn%20%20%3Cdiv%20class%3D%5C%22csl-entry%5C%22%3EKirby%2C%20R.%20L.%2C%20et%20al.%20%26%23x201C%3BCould%20Changes%20in%20the%20Wheelchair%20Delivery%20System%20Improve%20Safety%3F%26%23x201D%3B%20%3Ci%3ECMAJ%3A%20Canadian%20Medical%20Association%20Journal%3C%5C%2Fi%3E%2C%20vol.%20153%2C%20no.%2011%2C%20Dec.%201995%2C%20pp.%201585%26%23x2013%3B91%2C%20%3Ca%20href%3D%27https%3A%5C%2F%5C%2Fwww.ncbi.nlm.nih.gov%5C%2Fpmc%5C%2Farticles%5C%2FPMC1488010%5C%2F%27%3Ehttps%3A%5C%2F%5C%2Fwww.ncbi.nlm.nih.gov%5C%2Fpmc%5C%2Farticles%5C%2FPMC1488010%5C%2F%3C%5C%2Fa%3E.%3C%5C%2Fdiv%3E%5Cn%3C%5C%2Fdiv%3E%22%2C%22data%22%3A%7B%22itemType%22%3A%22journalArticle%22%2C%22title%22%3A%22Could%20changes%20in%20the%20wheelchair%20delivery%20system%20improve%20safety%3F%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22R%20L%22%2C%22lastName%22%3A%22Kirby%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22S%20G%22%2C%22lastName%22%3A%22Coughlan%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22M%22%2C%22lastName%22%3A%22Christie%22%7D%5D%2C%22abstractNote%22%3A%22Despite%20emerging%20evidence%20about%20the%20high%20incidence%20and%20severity%20of%20wheelchair-related%20injuries%2C%20regulations%20governing%20wheelchair%20safety%20are%20almost%20nonexistent%20in%20Canada.%20The%20authors%20believe%20that%2C%20to%20improve%20wheelchair%20safety%2C%20a%20concerted%20effort%20by%20government%2C%20manufacturers%2C%20purchasing%20groups%2C%20users%20and%20clinicians%20is%20needed.%20Health%20Canada%27s%20Health%20Protection%20Branch%20should%20treat%20wheelchairs%20as%20medical%20devices%20%28as%20defined%20in%20the%20Food%20and%20Drugs%20Act%201985%29%20and%20improve%20its%20injury-reporting%20network.%20Manufacturers%20should%20give%20a%20higher%20priority%20to%20safety%20in%20wheelchair%20design%2C%20improve%20their%20educational%20materials%20and%20formalize%20postmarketing%20surveillance.%20Purchasing%20groups%20should%20try%20to%20ensure%20that%20they%20do%20not%20stifle%20innovation%20in%20wheelchair%20design%20by%20setting%20unrealistic%20reimbursement%20ceilings%20and%20should%20use%20their%20market%20power%20more%20effectively.%20Users%20should%20obtain%20their%20wheelchairs%20in%20specialized%20settings%2C%20heed%20safety%20warnings%20and%20make%20more%20effective%20use%20of%20litigation%20when%20such%20action%20is%20warranted.%20Clinicians%20should%20ensure%20that%20patients%20are%20equipped%20with%20the%20most%20appropriate%20wheelchair%20for%20their%20needs%2C%20that%20they%20are%20given%20adequate%20training%20in%20safe%20wheelchair%20use%20and%20that%20they%20understand%20the%20dangers%20involved.%20Rapid%20changes%20in%20wheelchair%20technology%20and%20emerging%20evidence%20about%20the%20high%20incidence%20and%20severity%20of%20injuries%20related%20to%20wheelchair%20use%20suggest%20that%20such%20changes%20are%20needed%20in%20the%20wheelchair%20delivery%20system.%22%2C%22date%22%3A%221995-12-1%22%2C%22language%22%3A%22%22%2C%22DOI%22%3A%22%22%2C%22ISSN%22%3A%220820-3946%22%2C%22url%22%3A%22https%3A%5C%2F%5C%2Fwww.ncbi.nlm.nih.gov%5C%2Fpmc%5C%2Farticles%5C%2FPMC1488010%5C%2F%22%2C%22collections%22%3A%5B%22DD8I76K6%22%5D%2C%22dateModified%22%3A%222020-05-27T13%3A40%3A11Z%22%7D%7D%2C%7B%22key%22%3A%22FGZHSUNP%22%2C%22library%22%3A%7B%22id%22%3A6637697%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22Samuel%22%2C%22parsedDate%22%3A%222007%22%2C%22numChildren%22%3A0%7D%2C%22bib%22%3A%22%3Cdiv%20class%3D%5C%22csl-bib-body%5C%22%20style%3D%5C%22line-height%3A%202%3B%20padding-left%3A%202em%3B%20text-indent%3A-2em%3B%5C%22%3E%5Cn%20%20%3Cdiv%20class%3D%5C%22csl-entry%5C%22%3ESamuel%2C%20Andrew%2C%20editor.%20%26%23x201C%3BCases%20of%20Product%20Liability.%26%23x201D%3B%20%3Ci%3EThe%20Winning%20Line%3A%20A%20Forensic%20Engineer%26%23x2019%3Bs%20Casebook%3C%5C%2Fi%3E%2C%20Springer%2C%202007%2C%20pp.%20107%26%23x2013%3B74%2C%20doi%3A10.1007%5C%2F978-1-84628-097-9_3.%3C%5C%2Fdiv%3E%5Cn%3C%5C%2Fdiv%3E%22%2C%22data%22%3A%7B%22itemType%22%3A%22bookSection%22%2C%22title%22%3A%22Cases%20of%20Product%20Liability%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22editor%22%2C%22firstName%22%3A%22Andrew%22%2C%22lastName%22%3A%22Samuel%22%7D%5D%2C%22abstractNote%22%3A%223.10%20Chapter%20SummaryIn%20this%20chapter%20seven%20cases%20dealing%20with%20failures%20in%20technical%20contracting%20are%20presented.%20It%20is%20interesting%20to%20identify%20the%20common%20threads%20and%20issues%20that%20appear%20not%20only%20in%20these%20cases%20but%20in%20virtually%20all%20similar%20cases.%20In%20all%20of%20them%20the%20winning%20line%20was%20the%20capacity%20to%20recognise%20and%20draw%20out%20these%20issues.%20Issue%20%28a%29%20Failure%20of%20diligence%20in%20articulating%20and%20specifying%20product%20performance%20requirements%20expected%20from%20the%20product.%20Issue%20%28b%29%20Drafting%20defective%20technical%20contracts%20based%20on%20trust%20developed%20over%20long%20association%20with%20the%20supplier%20of%20technical%20service.%20In%20these%20cases%20Issue%20%28a%29%20is%20again%20commonly%20experienced.%20Issue%20%28c%29%20Failing%20to%20recognise%20the%20cooperative%20diligence%20essential%20to%20technical%20ventures%20where%20both%20supplier%20and%20client%20will%20benefit%20from%20such%20cooperation.%20Issue%20%28d%29%20Failure%20to%20recognise%20implicit%20%5Cu201csnake%20oil%5Cu201d%20promises%20such%20as%20%5Cu201ctrust%20us%2C%20we%20know%20what%20we%20are%20about%5Cu201d.%20In%20two%20cases%20complete%20technical%20expert%20reports%20are%20presented%20to%20indicate%20the%20format%20of%20such%20presentations.%22%2C%22bookTitle%22%3A%22The%20Winning%20Line%3A%20A%20Forensic%20Engineer%5Cu2019s%20Casebook%22%2C%22date%22%3A%222007%22%2C%22language%22%3A%22en%22%2C%22ISBN%22%3A%22978-1-84628-097-9%22%2C%22url%22%3A%22https%3A%5C%2F%5C%2Fdoi.org%5C%2F10.1007%5C%2F978-1-84628-097-9_3%22%2C%22collections%22%3A%5B%224EUQP96T%22%5D%2C%22dateModified%22%3A%222020-05-27T13%3A33%3A56Z%22%7D%7D%2C%7B%22key%22%3A%22RKQX32HG%22%2C%22library%22%3A%7B%22id%22%3A6637697%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22Keeton%22%2C%22parsedDate%22%3A%221964%22%2C%22numChildren%22%3A0%7D%2C%22bib%22%3A%22%3Cdiv%20class%3D%5C%22csl-bib-body%5C%22%20style%3D%5C%22line-height%3A%202%3B%20padding-left%3A%202em%3B%20text-indent%3A-2em%3B%5C%22%3E%5Cn%20%20%3Cdiv%20class%3D%5C%22csl-entry%5C%22%3EKeeton%2C%20Page.%20%26%23x201C%3BProducts%20Liability%20-%20The%20Nature%20and%20Extent%20of%20Strict%20Liability.%26%23x201D%3B%20%3Ci%3EUniversity%20of%20Illinois%20Law%20Forum%3C%5C%2Fi%3E%2C%20vol.%201964%2C%201964%2C%20p.%20693%2C%20%3Ca%20href%3D%27https%3A%5C%2F%5C%2Fheinonline.org%5C%2FHOL%5C%2FPage%3Fhandle%3Dhein.journals%5C%2Funilllr1964%26id%3D699%26div%3D%26collection%3D%27%3Ehttps%3A%5C%2F%5C%2Fheinonline.org%5C%2FHOL%5C%2FPage%3Fhandle%3Dhein.journals%5C%2Funilllr1964%26id%3D699%26div%3D%26collection%3D%3C%5C%2Fa%3E.%3C%5C%2Fdiv%3E%5Cn%3C%5C%2Fdiv%3E%22%2C%22data%22%3A%7B%22itemType%22%3A%22journalArticle%22%2C%22title%22%3A%22Products%20Liability%20-%20The%20Nature%20and%20Extent%20of%20Strict%20Liability%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Page%22%2C%22lastName%22%3A%22Keeton%22%7D%5D%2C%22abstractNote%22%3A%22%22%2C%22date%22%3A%221964%22%2C%22language%22%3A%22%22%2C%22DOI%22%3A%22%22%2C%22ISSN%22%3A%22%22%2C%22url%22%3A%22https%3A%5C%2F%5C%2Fheinonline.org%5C%2FHOL%5C%2FPage%3Fhandle%3Dhein.journals%5C%2Funilllr1964%26id%3D699%26div%3D%26collection%3D%22%2C%22collections%22%3A%5B%224EUQP96T%22%5D%2C%22dateModified%22%3A%222020-05-27T13%3A23%3A39Z%22%7D%7D%2C%7B%22key%22%3A%22EFQW9U6C%22%2C%22library%22%3A%7B%22id%22%3A6637697%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22Cooper%22%2C%22parsedDate%22%3A%221996-12-01%22%2C%22numChildren%22%3A0%7D%2C%22bib%22%3A%22%3Cdiv%20class%3D%5C%22csl-bib-body%5C%22%20style%3D%5C%22line-height%3A%202%3B%20padding-left%3A%202em%3B%20text-indent%3A-2em%3B%5C%22%3E%5Cn%20%20%3Cdiv%20class%3D%5C%22csl-entry%5C%22%3ECooper%2C%20Rory%20A.%20%26%23x201C%3BA%20Perspective%20on%20the%20Ultralight%20Wheelchair%20Revolution.%26%23x201D%3B%20%3Ci%3ETechnology%20and%20Disability%3C%5C%2Fi%3E%2C%20vol.%205%2C%20no.%203%26%23x2013%3B4%2C%20Dec.%201996%2C%20pp.%20383%26%23x2013%3B92%2C%20%3Ca%20href%3D%27http%3A%5C%2F%5C%2Fdoi.org%5C%2F10.3233%5C%2FTAD-1996-53-419%27%3Ehttp%3A%5C%2F%5C%2Fdoi.org%5C%2F10.3233%5C%2FTAD-1996-53-419%3C%5C%2Fa%3E.%3C%5C%2Fdiv%3E%5Cn%3C%5C%2Fdiv%3E%22%2C%22data%22%3A%7B%22itemType%22%3A%22journalArticle%22%2C%22title%22%3A%22A%20perspective%20on%20the%20ultralight%20wheelchair%20revolution%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Rory%20A.%22%2C%22lastName%22%3A%22Cooper%22%7D%5D%2C%22abstractNote%22%3A%22%22%2C%22date%22%3A%221996-12-01%22%2C%22language%22%3A%22%22%2C%22DOI%22%3A%2210.3233%5C%2FTAD-1996-53-419%22%2C%22ISSN%22%3A%221878643X%2C%2010554181%22%2C%22url%22%3A%22https%3A%5C%2F%5C%2Fwww.medra.org%5C%2Fservlet%5C%2FaliasResolver%3Falias%3Diospress%26doi%3D10.3233%5C%2FTAD-1996-53-419%22%2C%22collections%22%3A%5B%22DD8I76K6%22%5D%2C%22dateModified%22%3A%222020-05-27T13%3A20%3A26Z%22%7D%7D%2C%7B%22key%22%3A%22HIVSIC87%22%2C%22library%22%3A%7B%22id%22%3A6637697%7D%2C%22meta%22%3A%7B%22numChildren%22%3A1%7D%2C%22bib%22%3A%22%3Cdiv%20class%3D%5C%22csl-bib-body%5C%22%20style%3D%5C%22line-height%3A%202%3B%20padding-left%3A%202em%3B%20text-indent%3A-2em%3B%5C%22%3E%5Cn%20%20%3Cdiv%20class%3D%5C%22csl-entry%5C%22%3E%26%23x201C%3BWolturnus%20W5%20ADL%20rolstoel.%26%23x201D%3B%20%3Ci%3EDouble%20Performance%3C%5C%2Fi%3E%2C%20%3Ca%20href%3D%27https%3A%5C%2F%5C%2Fwww.doubleperformance.nl%5C%2Fproducten%5C%2Fadlrolstoelen%5C%2Fwolturnus-w5%5C%2F%27%3Ehttps%3A%5C%2F%5C%2Fwww.doubleperformance.nl%5C%2Fproducten%5C%2Fadlrolstoelen%5C%2Fwolturnus-w5%5C%2F%3C%5C%2Fa%3E.%20Accessed%2026%20May%202020.%3C%5C%2Fdiv%3E%5Cn%3C%5C%2Fdiv%3E%22%2C%22data%22%3A%7B%22itemType%22%3A%22blogPost%22%2C%22title%22%3A%22Wolturnus%20W5%20ADL%20rolstoel%22%2C%22creators%22%3A%5B%5D%2C%22abstractNote%22%3A%22De%20Wolturnus%20W5%20heeft%20een%20eigenzinnig%20Deens%20design.%5Cu00a0De%20W5%20kent%20een%20aantal%20varianten%20met%20elk%20specifieke%20eigenschappen.%20Bekijk%20de%5Cu00a0verschillende%20modellen.%22%2C%22blogTitle%22%3A%22Double%20Performance%22%2C%22date%22%3A%22%22%2C%22url%22%3A%22https%3A%5C%2F%5C%2Fwww.doubleperformance.nl%5C%2Fproducten%5C%2Fadlrolstoelen%5C%2Fwolturnus-w5%5C%2F%22%2C%22language%22%3A%22nl%22%2C%22collections%22%3A%5B%224EUQP96T%22%2C%22DD8I76K6%22%5D%2C%22dateModified%22%3A%222020-05-26T20%3A02%3A28Z%22%7D%7D%2C%7B%22key%22%3A%226SCGPKFK%22%2C%22library%22%3A%7B%22id%22%3A6637697%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22van%20Breukelen%22%2C%22parsedDate%22%3A%222010%22%2C%22numChildren%22%3A1%7D%2C%22bib%22%3A%22%3Cdiv%20class%3D%5C%22csl-bib-body%5C%22%20style%3D%5C%22line-height%3A%202%3B%20padding-left%3A%202em%3B%20text-indent%3A-2em%3B%5C%22%3E%5Cn%20%20%3Cdiv%20class%3D%5C%22csl-entry%5C%22%3Evan%20Breukelen%2C%20Kees.%20%26%23x201C%3BDe%20ergonomische%20zit%20deel%202.%26%23x201D%3B%20%3Ci%3ETijdschrift%20voor%20ergotherapie%3C%5C%2Fi%3E%2C%202010%2C%20p.%2020%2C%20%3Ca%20href%3D%27https%3A%5C%2F%5C%2Fdwarslaesie.nl%5C%2Fwp-content%5C%2Fuploads%5C%2F2016%5C%2F09%5C%2FDe-ergonomische-zit-Kees-van-Breukelen.pdf%27%3Ehttps%3A%5C%2F%5C%2Fdwarslaesie.nl%5C%2Fwp-content%5C%2Fuploads%5C%2F2016%5C%2F09%5C%2FDe-ergonomische-zit-Kees-van-Breukelen.pdf%3C%5C%2Fa%3E.%3C%5C%2Fdiv%3E%5Cn%3C%5C%2Fdiv%3E%22%2C%22data%22%3A%7B%22itemType%22%3A%22journalArticle%22%2C%22title%22%3A%22De%20ergonomische%20zit%20deel%202%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Kees%22%2C%22lastName%22%3A%22van%20Breukelen%22%7D%5D%2C%22abstractNote%22%3A%22%22%2C%22date%22%3A%222010%22%2C%22language%22%3A%22nl%22%2C%22DOI%22%3A%22%22%2C%22ISSN%22%3A%22%22%2C%22url%22%3A%22https%3A%5C%2F%5C%2Fdwarslaesie.nl%5C%2Fwp-content%5C%2Fuploads%5C%2F2016%5C%2F09%5C%2FDe-ergonomische-zit-Kees-van-Breukelen.pdf%22%2C%22collections%22%3A%5B%224EUQP96T%22%2C%22DD8I76K6%22%5D%2C%22dateModified%22%3A%222020-05-26T19%3A47%3A47Z%22%7D%7D%2C%7B%22key%22%3A%22SJBRCXZC%22%2C%22library%22%3A%7B%22id%22%3A6637697%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22Avan%22%2C%22parsedDate%22%3A%222020-05-26%22%2C%22numChildren%22%3A2%7D%2C%22bib%22%3A%22%3Cdiv%20class%3D%5C%22csl-bib-body%5C%22%20style%3D%5C%22line-height%3A%202%3B%20padding-left%3A%202em%3B%20text-indent%3A-2em%3B%5C%22%3E%5Cn%20%20%3Cdiv%20class%3D%5C%22csl-entry%5C%22%3EAvan.%20%26%23x201C%3BPer%201%20juli%202020%20nieuwe%20richtlijnen%20voor%20veilig%20rolstoelvervoer.%26%23x201D%3B%20%3Ci%3EAvan%3C%5C%2Fi%3E%2C%2026%20May%202020%2C%20%3Ca%20href%3D%27https%3A%5C%2F%5C%2Fwww.avan-vervoer.nl%5C%2Factueel%5C%2Fper-1-juli-nieuwe-richtlijnen-voor-veilig-rolstoelvervoer%5C%2F%27%3Ehttps%3A%5C%2F%5C%2Fwww.avan-vervoer.nl%5C%2Factueel%5C%2Fper-1-juli-nieuwe-richtlijnen-voor-veilig-rolstoelvervoer%5C%2F%3C%5C%2Fa%3E.%3C%5C%2Fdiv%3E%5Cn%3C%5C%2Fdiv%3E%22%2C%22data%22%3A%7B%22itemType%22%3A%22webpage%22%2C%22title%22%3A%22Per%201%20juli%202020%20nieuwe%20richtlijnen%20voor%20veilig%20rolstoelvervoer%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22%22%2C%22lastName%22%3A%22Avan%22%7D%5D%2C%22abstractNote%22%3A%22Avan%20brengt%20u%20waar%20u%20naartoe%20wilt%20in%20de%20regio%20Arnhem-Nijmegen.%20Wilt%20u%20naar%20uw%20dagbesteding%3F%20Naar%20de%20markt%3F%20Naar%20school%3F%20Naar%20zwemles%20of%20de%20kleinkinderen%3F%22%2C%22date%22%3A%222020-05-26%22%2C%22url%22%3A%22https%3A%5C%2F%5C%2Fwww.avan-vervoer.nl%5C%2Factueel%5C%2Fper-1-juli-nieuwe-richtlijnen-voor-veilig-rolstoelvervoer%5C%2F%22%2C%22language%22%3A%22nl%22%2C%22collections%22%3A%5B%224EUQP96T%22%5D%2C%22dateModified%22%3A%222020-05-26T15%3A08%3A52Z%22%7D%7D%2C%7B%22key%22%3A%22DFD8MRC7%22%2C%22library%22%3A%7B%22id%22%3A6637697%7D%2C%22meta%22%3A%7B%22numChildren%22%3A1%7D%2C%22bib%22%3A%22%3Cdiv%20class%3D%5C%22csl-bib-body%5C%22%20style%3D%5C%22line-height%3A%202%3B%20padding-left%3A%202em%3B%20text-indent%3A-2em%3B%5C%22%3E%5Cn%20%20%3Cdiv%20class%3D%5C%22csl-entry%5C%22%3E%3Ci%3ENieuwsbrief%204%2C%20November%202019%20%7C%20Avan%3C%5C%2Fi%3E.%20%3Ca%20href%3D%27https%3A%5C%2F%5C%2Fwww.avan-vervoer.nl%5C%2Factueel%5C%2Fnieuwsbrief-4-november-2019%5C%2F%27%3Ehttps%3A%5C%2F%5C%2Fwww.avan-vervoer.nl%5C%2Factueel%5C%2Fnieuwsbrief-4-november-2019%5C%2F%3C%5C%2Fa%3E.%20Accessed%2026%20May%202020.%3C%5C%2Fdiv%3E%5Cn%3C%5C%2Fdiv%3E%22%2C%22data%22%3A%7B%22itemType%22%3A%22webpage%22%2C%22title%22%3A%22Nieuwsbrief%204%2C%20november%202019%20%7C%20Avan%22%2C%22creators%22%3A%5B%5D%2C%22abstractNote%22%3A%22%22%2C%22date%22%3A%22%22%2C%22url%22%3A%22https%3A%5C%2F%5C%2Fwww.avan-vervoer.nl%5C%2Factueel%5C%2Fnieuwsbrief-4-november-2019%5C%2F%22%2C%22language%22%3A%22%22%2C%22collections%22%3A%5B%224EUQP96T%22%5D%2C%22dateModified%22%3A%222020-05-26T15%3A06%3A36Z%22%7D%7D%2C%7B%22key%22%3A%22FI3GAGPQ%22%2C%22library%22%3A%7B%22id%22%3A6637697%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22Markt%22%2C%22parsedDate%22%3A%222010-12-10%22%2C%22numChildren%22%3A3%7D%2C%22bib%22%3A%22%3Cdiv%20class%3D%5C%22csl-bib-body%5C%22%20style%3D%5C%22line-height%3A%202%3B%20padding-left%3A%202em%3B%20text-indent%3A-2em%3B%5C%22%3E%5Cn%20%20%3Cdiv%20class%3D%5C%22csl-entry%5C%22%3EMarkt%2C%20Autoriteit%20Consument%20%26amp%3B.%20%3Ci%3EACM%20Nordic%20Capital%20-%20Handicare%20concentratiebesluit%20%7C%20ACM.nl%3C%5C%2Fi%3E.%2010%20Dec.%202010%2C%20%3Ca%20href%3D%27https%3A%5C%2F%5C%2Fwww.acm.nl%5C%2Fnl%5C%2Fpublicaties%5C%2Fpublicatie%5C%2F2507%5C%2FNordic-Capital---Handicare-concentratiebesluit%27%3Ehttps%3A%5C%2F%5C%2Fwww.acm.nl%5C%2Fnl%5C%2Fpublicaties%5C%2Fpublicatie%5C%2F2507%5C%2FNordic-Capital---Handicare-concentratiebesluit%3C%5C%2Fa%3E.%3C%5C%2Fdiv%3E%5Cn%3C%5C%2Fdiv%3E%22%2C%22data%22%3A%7B%22itemType%22%3A%22webpage%22%2C%22title%22%3A%22ACM%20Nordic%20Capital%20-%20Handicare%20concentratiebesluit%20%7C%20ACM.nl%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Autoriteit%20Consument%20%26%22%2C%22lastName%22%3A%22Markt%22%7D%5D%2C%22abstractNote%22%3A%22De%20Nederlandse%20Mededingingsautoriteit%20%28NMa%29%20stelt%20voorwaarden%20aan%20de%20overname%20van%20Handicare%20door%20Nordic%20Capital.%20Handicare%20moet%20een%20substantieel%20deel%20van%20haar%20productie%2C%20distributi%22%2C%22date%22%3A%222010-12-10%22%2C%22url%22%3A%22https%3A%5C%2F%5C%2Fwww.acm.nl%5C%2Fnl%5C%2Fpublicaties%5C%2Fpublicatie%5C%2F2507%5C%2FNordic-Capital---Handicare-concentratiebesluit%22%2C%22language%22%3A%22nl%22%2C%22collections%22%3A%5B%224EUQP96T%22%5D%2C%22dateModified%22%3A%222020-05-26T14%3A57%3A12Z%22%7D%7D%2C%7B%22key%22%3A%224W2QPJQ3%22%2C%22library%22%3A%7B%22id%22%3A6637697%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22Markt%22%2C%22numChildren%22%3A2%7D%2C%22bib%22%3A%22%3Cdiv%20class%3D%5C%22csl-bib-body%5C%22%20style%3D%5C%22line-height%3A%202%3B%20padding-left%3A%202em%3B%20text-indent%3A-2em%3B%5C%22%3E%5Cn%20%20%3Cdiv%20class%3D%5C%22csl-entry%5C%22%3EMarkt%2C%20Autoriteit%20Consument%20%26amp%3B.%20%3Ci%3EACM%20wijzigt%20vergunningsbesluit%20overname%20Handicare%20door%20Nordic%20Capital%20%7C%20ACM.nl%3C%5C%2Fi%3E.%20%5C%2F%2C%20%3Ca%20href%3D%27https%3A%5C%2F%5C%2Fwww.acm.nl%5C%2Fnl%5C%2Fpublicaties%5C%2Fpublicatie%5C%2F13086%5C%2FACM-wijzigt-vergunningsbesluit-overname-Handicare-door-Nordic-Capital%27%3Ehttps%3A%5C%2F%5C%2Fwww.acm.nl%5C%2Fnl%5C%2Fpublicaties%5C%2Fpublicatie%5C%2F13086%5C%2FACM-wijzigt-vergunningsbesluit-overname-Handicare-door-Nordic-Capital%3C%5C%2Fa%3E.%3C%5C%2Fdiv%3E%5Cn%3C%5C%2Fdiv%3E%22%2C%22data%22%3A%7B%22itemType%22%3A%22webpage%22%2C%22title%22%3A%22ACM%20wijzigt%20vergunningsbesluit%20overname%20Handicare%20door%20Nordic%20Capital%20%7C%20ACM.nl%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Autoriteit%20Consument%20%26%22%2C%22lastName%22%3A%22Markt%22%7D%5D%2C%22abstractNote%22%3A%22ACM%20wijzigt%20op%20verzoek%20van%20Noric%20Capital%20het%20vergunningsbesluit%20van%2010%20december%202010%20over%20de%20overname%20van%20Handicare%20door%20Nordic%20Capital.%22%2C%22date%22%3A%22%5C%2F%22%2C%22url%22%3A%22https%3A%5C%2F%5C%2Fwww.acm.nl%5C%2Fnl%5C%2Fpublicaties%5C%2Fpublicatie%5C%2F13086%5C%2FACM-wijzigt-vergunningsbesluit-overname-Handicare-door-Nordic-Capital%22%2C%22language%22%3A%22nl%22%2C%22collections%22%3A%5B%224EUQP96T%22%5D%2C%22dateModified%22%3A%222020-05-26T14%3A52%3A45Z%22%7D%7D%2C%7B%22key%22%3A%22LLVSDDQ4%22%2C%22library%22%3A%7B%22id%22%3A6637697%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22Markt%22%2C%22parsedDate%22%3A%222019-03-22%22%2C%22numChildren%22%3A2%7D%2C%22bib%22%3A%22%3Cdiv%20class%3D%5C%22csl-bib-body%5C%22%20style%3D%5C%22line-height%3A%202%3B%20padding-left%3A%202em%3B%20text-indent%3A-2em%3B%5C%22%3E%5Cn%20%20%3Cdiv%20class%3D%5C%22csl-entry%5C%22%3EMarkt%2C%20Autoriteit%20Consument%20%26amp%3B.%20%3Ci%3ENordic%20Capital%20mag%20Conscia%20overnemen%20%28concentratiebesluit%29%20%7C%20ACM.nl%3C%5C%2Fi%3E.%2022%20Mar.%202019%2C%20%3Ca%20href%3D%27https%3A%5C%2F%5C%2Fwww.acm.nl%5C%2Fnl%5C%2Fpublicaties%5C%2Fnordic-capital-mag-conscia-overnemen-concentratiebesluit%27%3Ehttps%3A%5C%2F%5C%2Fwww.acm.nl%5C%2Fnl%5C%2Fpublicaties%5C%2Fnordic-capital-mag-conscia-overnemen-concentratiebesluit%3C%5C%2Fa%3E.%3C%5C%2Fdiv%3E%5Cn%3C%5C%2Fdiv%3E%22%2C%22data%22%3A%7B%22itemType%22%3A%22webpage%22%2C%22title%22%3A%22Nordic%20Capital%20mag%20Conscia%20overnemen%20%28concentratiebesluit%29%20%7C%20ACM.nl%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Autoriteit%20Consument%20%26%22%2C%22lastName%22%3A%22Markt%22%7D%5D%2C%22abstractNote%22%3A%22Nordic%20Capital%20mag%20Conscia%20overnemen.%20Dat%20heeft%20de%20ACM%20op%2021%20maart%202019%20besloten.%22%2C%22date%22%3A%222019-03-22%22%2C%22url%22%3A%22https%3A%5C%2F%5C%2Fwww.acm.nl%5C%2Fnl%5C%2Fpublicaties%5C%2Fnordic-capital-mag-conscia-overnemen-concentratiebesluit%22%2C%22language%22%3A%22nl%22%2C%22collections%22%3A%5B%224EUQP96T%22%5D%2C%22dateModified%22%3A%222020-05-26T14%3A42%3A27Z%22%7D%7D%2C%7B%22key%22%3A%22GLABHZKE%22%2C%22library%22%3A%7B%22id%22%3A6637697%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22VdT%5Cu00dcV%22%2C%22parsedDate%22%3A%222013-09-01%22%2C%22numChildren%22%3A2%7D%2C%22bib%22%3A%22%3Cdiv%20class%3D%5C%22csl-bib-body%5C%22%20style%3D%5C%22line-height%3A%202%3B%20padding-left%3A%202em%3B%20text-indent%3A-2em%3B%5C%22%3E%5Cn%20%20%3Cdiv%20class%3D%5C%22csl-entry%5C%22%3EVdT%26%23xDC%3BV.%20%3Ci%3ELegal%20Compliance%20for%20the%20Transportation%20of%20Wheelchair%20Users%20Policy%20Document%20of%20the%20Roundtable%20%26%23x201C%3BSafe%20Mobility%20for%20People%20with%20Disabilities.%26%23x201D%3B%3C%5C%2Fi%3E%20VdT%26%23xDC%3BV%2C%201%20Sept.%202013%2C%20%3Ca%20href%3D%27https%3A%5C%2F%5C%2Fwww.vdtuev.de%5C%2Fdok_view%3Foid%3D388608%27%3Ehttps%3A%5C%2F%5C%2Fwww.vdtuev.de%5C%2Fdok_view%3Foid%3D388608%3C%5C%2Fa%3E.%3C%5C%2Fdiv%3E%5Cn%3C%5C%2Fdiv%3E%22%2C%22data%22%3A%7B%22itemType%22%3A%22document%22%2C%22title%22%3A%22Legal%20compliance%20for%20the%20transportation%20of%20wheelchair%20users%20Policy%20Document%20of%20the%20roundtable%20%5Cu201cSafe%20mobility%20for%20people%20with%20disabilities%5Cu201d%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22name%22%3A%22VdT%5Cu00dcV%22%7D%5D%2C%22abstractNote%22%3A%22%22%2C%22date%22%3A%229-1-2013%22%2C%22language%22%3A%22en%22%2C%22url%22%3A%22https%3A%5C%2F%5C%2Fwww.vdtuev.de%5C%2Fdok_view%3Foid%3D388608%22%2C%22collections%22%3A%5B%224EUQP96T%22%5D%2C%22dateModified%22%3A%222020-05-26T14%3A18%3A12Z%22%7D%7D%2C%7B%22key%22%3A%22QRAD85LN%22%2C%22library%22%3A%7B%22id%22%3A6637697%7D%2C%22meta%22%3A%7B%22numChildren%22%3A0%7D%2C%22bib%22%3A%22%3Cdiv%20class%3D%5C%22csl-bib-body%5C%22%20style%3D%5C%22line-height%3A%202%3B%20padding-left%3A%202em%3B%20text-indent%3A-2em%3B%5C%22%3E%5Cn%20%20%3Cdiv%20class%3D%5C%22csl-entry%5C%22%3E%3Ci%3EMedien-Center%20-%20Sichere%20Bef%26%23xF6%3Brderung%20von%20Menschen%20Mit%20Behinderungen%20-%20BGW-Online%3C%5C%2Fi%3E.%20%3Ca%20href%3D%27https%3A%5C%2F%5C%2Fwww.bgw-online.de%5C%2FDE%5C%2FMedien-Service%5C%2FMedien-Center%5C%2FMedientypen%5C%2FBGW-Broschueren%5C%2FBGW05-11-003_Sichere-Befoerderung-von-Menschen-mit-Behinderungen.html%27%3Ehttps%3A%5C%2F%5C%2Fwww.bgw-online.de%5C%2FDE%5C%2FMedien-Service%5C%2FMedien-Center%5C%2FMedientypen%5C%2FBGW-Broschueren%5C%2FBGW05-11-003_Sichere-Befoerderung-von-Menschen-mit-Behinderungen.html%3C%5C%2Fa%3E.%20Accessed%2026%20May%202020.%3C%5C%2Fdiv%3E%5Cn%3C%5C%2Fdiv%3E%22%2C%22data%22%3A%7B%22itemType%22%3A%22webpage%22%2C%22title%22%3A%22Medien-Center%20-%20Sichere%20Bef%5Cu00f6rderung%20von%20Menschen%20mit%20Behinderungen%20-%20BGW-online%22%2C%22creators%22%3A%5B%5D%2C%22abstractNote%22%3A%22%22%2C%22date%22%3A%22%22%2C%22url%22%3A%22https%3A%5C%2F%5C%2Fwww.bgw-online.de%5C%2FDE%5C%2FMedien-Service%5C%2FMedien-Center%5C%2FMedientypen%5C%2FBGW-Broschueren%5C%2FBGW05-11-003_Sichere-Befoerderung-von-Menschen-mit-Behinderungen.html%22%2C%22language%22%3A%22%22%2C%22collections%22%3A%5B%224EUQP96T%22%5D%2C%22dateModified%22%3A%222020-05-26T14%3A00%3A59Z%22%7D%7D%2C%7B%22key%22%3A%22C9UGBTZH%22%2C%22library%22%3A%7B%22id%22%3A6637697%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22Veenbaas%22%2C%22parsedDate%22%3A%222003%22%2C%22numChildren%22%3A1%7D%2C%22bib%22%3A%22%3Cdiv%20class%3D%5C%22csl-bib-body%5C%22%20style%3D%5C%22line-height%3A%202%3B%20padding-left%3A%202em%3B%20text-indent%3A-2em%3B%5C%22%3E%5Cn%20%20%3Cdiv%20class%3D%5C%22csl-entry%5C%22%3EVeenbaas%2C%20Roelof.%20%3Ci%3ETNO-rapport%20rolstoelvervoer.pdf%3C%5C%2Fi%3E.%2003.OR.AC.048.1%5C%2FROV%2C%20TNO%20Wegtransportmiddelen%2C%20oktober%202003%2C%20p.%2028.%3C%5C%2Fdiv%3E%5Cn%3C%5C%2Fdiv%3E%22%2C%22data%22%3A%7B%22itemType%22%3A%22report%22%2C%22title%22%3A%22TNO-rapport%20rolstoelvervoer.pdf%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Roelof%22%2C%22lastName%22%3A%22Veenbaas%22%7D%5D%2C%22abstractNote%22%3A%22Het%20Ministerie%20van%20Verkeer%20en%20Waterstaat%20onderkent%20ten%20zeerste%20de%20noodzaak%20aandacht%5Cnte%20schenken%20aan%20de%20veiligheid%20van%20rolstoelgebruikers%20in%20het%20verkeer%20en%20vervoer.%20Daarom%5Cnis%20besloten%2C%20naast%20een%20inventarisatie%20van%20de%20internationale%20regelgeving%20en%20literatuur%20op%5Cnhet%20gebied%20van%20het%20rolstoelvervoer%2C%20tevens%20een%20meldpunt%20en%20een%20meldingsprocedure%20van%5Cn%28bijna%29%20ongevallen%20van%20het%20rolstoelvervoer%20in%20%28collectieve%5C%2F%20openbare%29%20vervoersystemen%20in%5Cnhet%20leven%20te%20roepen.%5CnOp%2017%20december%202001%20is%20daartoe%20op%20de%20site%20www.leefwijzer.nl%5C%5Crolstoelvervoer%20een%20meldingsformulier%5Cnbeschikbaar%20gesteld.%20Een%20papieren%20versie%20was%20tegelijkertijd%20op%20te%20vragen%5Cnbij%20TNO-WT.%20Tegelijkertijd%20werd%20in%20een%20persbericht%20aandacht%20besteed%20aan%20het%20openen%5Cnvan%20de%20site.%5CnHet%20meldingsformulier%20was%20bedoeld%20voor%20alle%20rolstoelvervoersituaties%20%28taxi%2C%20bus%2C%20tram%2C%5Cnmetro%2C%20light%20rail%2C%20trein%29%20over%20land.%20Het%20overgrote%20deel%20van%20de%20meldingen%20betrof%20echter%5Cntaxibusvervoer%20als%20gehandicaptenvervoer%2C%20ziekenvervoer%2C%20leerlingenvervoer%20en%20woonwerkverkeer.%5CnVanaf%20half%20december%202001%20tot%20eind%20mei%202003%20kwamen%20er%2083%20meldingen%20binnen%20met%20betrekking%5Cntot%20onveilige%20situaties%20en%20%28bijna%29%20ongevallen.%20Er%20gaapt%20een%20kloof%20tussen%20het%20convenant%5CnVeilig%20Vervoer%20Rolstoelinzittenden%2C%20waarin%20o.a.%20de%20VNG%2C%20KNV%20taxi%20en%20CG-raad%5Cnafspraken%20hebben%20gemaakt%2C%20over%20de%20toegankelijkheid%20en%20veiligheid%20van%20het%20rolstoelvervoer%2C%5Cnen%20de%20situatie%20in%20de%20praktijk.%22%2C%22reportNumber%22%3A%2203.OR.AC.048.1%5C%2FROV%22%2C%22reportType%22%3A%22%22%2C%22institution%22%3A%22TNO%20Wegtransportmiddelen%22%2C%22date%22%3A%2216%20oktober%202003%22%2C%22language%22%3A%22nl-NL%22%2C%22url%22%3A%22%22%2C%22collections%22%3A%5B%224EUQP96T%22%5D%2C%22dateModified%22%3A%222020-05-26T12%3A43%3A00Z%22%7D%7D%2C%7B%22key%22%3A%22FPSHMV7K%22%2C%22library%22%3A%7B%22id%22%3A6637697%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22AMF-Bruns%22%2C%22numChildren%22%3A0%7D%2C%22bib%22%3A%22%3Cdiv%20class%3D%5C%22csl-bib-body%5C%22%20style%3D%5C%22line-height%3A%202%3B%20padding-left%3A%202em%3B%20text-indent%3A-2em%3B%5C%22%3E%5Cn%20%20%3Cdiv%20class%3D%5C%22csl-entry%5C%22%3EAMF-Bruns.%20%26%23x201C%3BDer%20Kraftknotenadapter%20%7C%20Personen-%20%26amp%3B%20Rollstuhlsicherung%20im%20Fahrzeug.%26%23x201D%3B%20%3Ci%3EDer%20Kraftknoten%20-%20Das%20Plus%20an%20Sicherheit%3C%5C%2Fi%3E%2C%20%3Ca%20href%3D%27http%3A%5C%2F%5C%2Fwww.kraftknotenadapter.de%5C%2F%27%3Ehttp%3A%5C%2F%5C%2Fwww.kraftknotenadapter.de%5C%2F%3C%5C%2Fa%3E.%20Accessed%2024%20May%202020.%3C%5C%2Fdiv%3E%5Cn%3C%5C%2Fdiv%3E%22%2C%22data%22%3A%7B%22itemType%22%3A%22webpage%22%2C%22title%22%3A%22Der%20Kraftknotenadapter%20%7C%20Personen-%20%26%20Rollstuhlsicherung%20im%20Fahrzeug%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22name%22%3A%22AMF-Bruns%22%7D%5D%2C%22abstractNote%22%3A%22Kraftknoten%20System%20zur%20Sicherung%20von%20Personen%20und%20Rollst%5Cu00fchlen%20im%20Fahrzeug%20%5Cu2022%20AMF-Bruns%20Kraftknotenadapter%20ist%20getestet%20%26%20gezogen%20gem%5Cu00e4%5Cu00df%20DIN%2075078-2%20%5Cu2713%22%2C%22date%22%3A%22%22%2C%22url%22%3A%22http%3A%5C%2F%5C%2Fwww.kraftknotenadapter.de%5C%2F%22%2C%22language%22%3A%22de-DE%22%2C%22collections%22%3A%5B%224EUQP96T%22%2C%22DD8I76K6%22%5D%2C%22dateModified%22%3A%222020-05-26T12%3A33%3A45Z%22%7D%7D%2C%7B%22key%22%3A%227NKUVQX2%22%2C%22library%22%3A%7B%22id%22%3A6637697%7D%2C%22meta%22%3A%7B%22parsedDate%22%3A%222017%22%2C%22numChildren%22%3A1%7D%2C%22bib%22%3A%22%3Cdiv%20class%3D%5C%22csl-bib-body%5C%22%20style%3D%5C%22line-height%3A%202%3B%20padding-left%3A%202em%3B%20text-indent%3A-2em%3B%5C%22%3E%5Cn%20%20%3Cdiv%20class%3D%5C%22csl-entry%5C%22%3E%3Ci%3EConvenant%20samengesteld%20product%3C%5C%2Fi%3E.%20Firevaned%2C%20oktober%202017.%3C%5C%2Fdiv%3E%5Cn%3C%5C%2Fdiv%3E%22%2C%22data%22%3A%7B%22itemType%22%3A%22document%22%2C%22title%22%3A%22Convenant%20samengesteld%20product%22%2C%22creators%22%3A%5B%5D%2C%22abstractNote%22%3A%22%22%2C%22date%22%3A%22oktober%202017%22%2C%22language%22%3A%22nl-NL%22%2C%22url%22%3A%22%22%2C%22collections%22%3A%5B%224EUQP96T%22%5D%2C%22dateModified%22%3A%222020-05-26T12%3A05%3A24Z%22%7D%7D%2C%7B%22key%22%3A%22YSUZEF5F%22%2C%22library%22%3A%7B%22id%22%3A6637697%7D%2C%22meta%22%3A%7B%22parsedDate%22%3A%222010-03-26%22%2C%22numChildren%22%3A1%7D%2C%22bib%22%3A%22%3Cdiv%20class%3D%5C%22csl-bib-body%5C%22%20style%3D%5C%22line-height%3A%202%3B%20padding-left%3A%202em%3B%20text-indent%3A-2em%3B%5C%22%3E%5Cn%20%20%3Cdiv%20class%3D%5C%22csl-entry%5C%22%3E%3Ci%3E20100326%20Study%20into%20Occupant%20Restraint%20Path%20in%20Custom%20Seating.Pdf%3C%5C%2Fi%3E.%20Coventry%20University%2C%20Faculty%20of%20Engineering%2C%2026%20Mar.%202010%2C%20%3Ca%20href%3D%27https%3A%5C%2F%5C%2Fwww.pmguk.co.uk%5C%2Fdata%5C%2Fpage_files%5C%2FBest%2520Practice%5C%2Fstudy%2520into%2520occupant%2520restraint%2520path%2520in%2520custom%2520seating.pdf%27%3Ehttps%3A%5C%2F%5C%2Fwww.pmguk.co.uk%5C%2Fdata%5C%2Fpage_files%5C%2FBest%2520Practice%5C%2Fstudy%2520into%2520occupant%2520restraint%2520path%2520in%2520custom%2520seating.pdf%3C%5C%2Fa%3E.%3C%5C%2Fdiv%3E%5Cn%3C%5C%2Fdiv%3E%22%2C%22data%22%3A%7B%22itemType%22%3A%22document%22%2C%22title%22%3A%2220100326%20Study%20into%20occupant%20restraint%20path%20in%20custom%20seating.pdf%22%2C%22creators%22%3A%5B%5D%2C%22abstractNote%22%3A%22%22%2C%22date%22%3A%2226-03-2010%22%2C%22language%22%3A%22en%22%2C%22url%22%3A%22https%3A%5C%2F%5C%2Fwww.pmguk.co.uk%5C%2Fdata%5C%2Fpage_files%5C%2FBest%2520Practice%5C%2Fstudy%2520into%2520occupant%2520restraint%2520path%2520in%2520custom%2520seating.pdf%22%2C%22collections%22%3A%5B%224EUQP96T%22%5D%2C%22dateModified%22%3A%222020-05-26T12%3A01%3A26Z%22%7D%7D%2C%7B%22key%22%3A%22K7DPE4N3%22%2C%22library%22%3A%7B%22id%22%3A6637697%7D%2C%22meta%22%3A%7B%22numChildren%22%3A1%7D%2C%22bib%22%3A%22%3Cdiv%20class%3D%5C%22csl-bib-body%5C%22%20style%3D%5C%22line-height%3A%202%3B%20padding-left%3A%202em%3B%20text-indent%3A-2em%3B%5C%22%3E%5Cn%20%20%3Cdiv%20class%3D%5C%22csl-entry%5C%22%3E%3Ci%3EKerncijfers%20zorgvervoer%202017%3C%5C%2Fi%3E.%20Panteia%2C%20p.%2010%2C%20%3Ca%20href%3D%27https%3A%5C%2F%5C%2Fai-mobiliteit.nl%5C%2F%27%3Ehttps%3A%5C%2F%5C%2Fai-mobiliteit.nl%5C%2F%3C%5C%2Fa%3E.%20Accessed%2025%20May%202020.%3C%5C%2Fdiv%3E%5Cn%3C%5C%2Fdiv%3E%22%2C%22data%22%3A%7B%22itemType%22%3A%22report%22%2C%22title%22%3A%22Kerncijfers%20zorgvervoer%202017%22%2C%22creators%22%3A%5B%5D%2C%22abstractNote%22%3A%22KNV%20Taxi%2C%20FNV%20Taxi%20en%20CNV%20Vakmensen%20hebben%20de%20handen%20ineen%20geslagen%20en%20het%20Aanbestedingsinstituut%20Mobiliteit%20%28AIM%29%20opgericht.%22%2C%22reportNumber%22%3A%22%22%2C%22reportType%22%3A%22%22%2C%22institution%22%3A%22Panteia%22%2C%22date%22%3A%22%22%2C%22language%22%3A%22nl%22%2C%22url%22%3A%22https%3A%5C%2F%5C%2Fai-mobiliteit.nl%5C%2F%22%2C%22collections%22%3A%5B%224EUQP96T%22%5D%2C%22dateModified%22%3A%222020-05-26T11%3A50%3A22Z%22%7D%7D%2C%7B%22key%22%3A%22SS6SNSMP%22%2C%22library%22%3A%7B%22id%22%3A6637697%7D%2C%22meta%22%3A%7B%22numChildren%22%3A0%7D%2C%22bib%22%3A%22%3Cdiv%20class%3D%5C%22csl-bib-body%5C%22%20style%3D%5C%22line-height%3A%202%3B%20padding-left%3A%202em%3B%20text-indent%3A-2em%3B%5C%22%3E%5Cn%20%20%3Cdiv%20class%3D%5C%22csl-entry%5C%22%3E%3Ci%3EAanbestedingsinstituut%20Mobiliteit%3C%5C%2Fi%3E.%20%3Ca%20href%3D%27https%3A%5C%2F%5C%2Fai-mobiliteit.nl%5C%2F%27%3Ehttps%3A%5C%2F%5C%2Fai-mobiliteit.nl%5C%2F%3C%5C%2Fa%3E.%20Accessed%2025%20May%202020.%3C%5C%2Fdiv%3E%5Cn%3C%5C%2Fdiv%3E%22%2C%22data%22%3A%7B%22itemType%22%3A%22webpage%22%2C%22title%22%3A%22Aanbestedingsinstituut%20Mobiliteit%22%2C%22creators%22%3A%5B%5D%2C%22abstractNote%22%3A%22KNV%20Taxi%2C%20FNV%20Taxi%20en%20CNV%20Vakmensen%20hebben%20de%20handen%20ineen%20geslagen%20en%20het%20Aanbestedingsinstituut%20Mobiliteit%20%28AIM%29%20opgericht.%22%2C%22date%22%3A%22%22%2C%22url%22%3A%22https%3A%5C%2F%5C%2Fai-mobiliteit.nl%5C%2F%22%2C%22language%22%3A%22nl%22%2C%22collections%22%3A%5B%224EUQP96T%22%5D%2C%22dateModified%22%3A%222020-05-26T11%3A46%3A46Z%22%7D%7D%2C%7B%22key%22%3A%22HSIAT47I%22%2C%22library%22%3A%7B%22id%22%3A6637697%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22Kirkels%22%2C%22numChildren%22%3A1%7D%2C%22bib%22%3A%22%3Cdiv%20class%3D%5C%22csl-bib-body%5C%22%20style%3D%5C%22line-height%3A%202%3B%20padding-left%3A%202em%3B%20text-indent%3A-2em%3B%5C%22%3E%5Cn%20%20%3Cdiv%20class%3D%5C%22csl-entry%5C%22%3EKirkels%2C%20A.%20F.%20%3Ci%3EGehandicapten%20en%20ouderen%20deur-tot-deur%20vervoer%3C%5C%2Fi%3E.%20p.%2045.%3C%5C%2Fdiv%3E%5Cn%3C%5C%2Fdiv%3E%22%2C%22data%22%3A%7B%22itemType%22%3A%22journalArticle%22%2C%22title%22%3A%22Gehandicapten%20en%20ouderen%20deur-tot-deur%20vervoer%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22A%20F%22%2C%22lastName%22%3A%22Kirkels%22%7D%5D%2C%22abstractNote%22%3A%22%22%2C%22date%22%3A%22%22%2C%22language%22%3A%22nl%22%2C%22DOI%22%3A%22%22%2C%22ISSN%22%3A%22%22%2C%22url%22%3A%22%22%2C%22collections%22%3A%5B%224EUQP96T%22%5D%2C%22dateModified%22%3A%222020-05-26T11%3A42%3A42Z%22%7D%7D%2C%7B%22key%22%3A%22NSQ7F6B4%22%2C%22library%22%3A%7B%22id%22%3A6637697%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22Buiren%20et%20al.%22%2C%22parsedDate%22%3A%222016%22%2C%22numChildren%22%3A1%7D%2C%22bib%22%3A%22%3Cdiv%20class%3D%5C%22csl-bib-body%5C%22%20style%3D%5C%22line-height%3A%202%3B%20padding-left%3A%202em%3B%20text-indent%3A-2em%3B%5C%22%3E%5Cn%20%20%3Cdiv%20class%3D%5C%22csl-entry%5C%22%3EBuiren%2C%20Koert%20van%2C%20et%20al.%20%3Ci%3EDe%20vloek%20van%20de%20winnende%20taxi%3A%20onderzoek%20naar%20het%20probleem%20van%20te%20lage%20biedingen%20bij%20aanbestedingen%20in%20het%20doelgroepenvervoer%3C%5C%2Fi%3E.%202016.%3C%5C%2Fdiv%3E%5Cn%3C%5C%2Fdiv%3E%22%2C%22data%22%3A%7B%22itemType%22%3A%22book%22%2C%22title%22%3A%22De%20vloek%20van%20de%20winnende%20taxi%3A%20onderzoek%20naar%20het%20probleem%20van%20te%20lage%20biedingen%20bij%20aanbestedingen%20in%20het%20doelgroepenvervoer%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Koert%20van%22%2C%22lastName%22%3A%22Buiren%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Julie%22%2C%22lastName%22%3A%22Fijnje%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Daan%20in%20%27t%22%2C%22lastName%22%3A%22Veld%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22name%22%3A%22SEO%20Economisch%20Onderzoek%20%28Amsterdam%29%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22name%22%3A%22KNV%20Taxi%22%7D%5D%2C%22abstractNote%22%3A%22%22%2C%22date%22%3A%222016%22%2C%22language%22%3A%22nl%22%2C%22ISBN%22%3A%22978-90-6733-833-2%22%2C%22url%22%3A%22%22%2C%22collections%22%3A%5B%224EUQP96T%22%5D%2C%22dateModified%22%3A%222020-05-26T11%3A42%3A40Z%22%7D%7D%5D%7D
Vocht, Sven de, et al. Lead companies: van familiebedrijf tot multinational . Lannoo Meulenhoff - Belgium, 2016.
Vries, Judith F. A. de. De toekomst van de ‘open’ ambtenaar . Universiteit Utrcht, Faculteit Rebo, 22 Aug. 2019.
Koninkrijksrelaties, Ministerie van Binnenlandse Zaken en.
Reglement verkeersregels en verkeerstekens 1990 (RVV 1990) . 1990,
https://wetten.overheid.nl/BWBR0004825/2020-01-01/#HoofdstukII_Paragraaf27_Artikel59 .
Orton, Nicole R.
Ride Safe Brochures . University of Michigan Transportation Research Institute (UMTRI), 5 July 2019,
http://wc-transportation-safety.umtri.umich.edu/ridesafe-brochure .
Schneider, Lawrence W., et al.
Wheelchair Occupant Studies . Final Report, 2016–8, University of Michigan Transportation Research Institute (UMTRI), July 2016, p. 199,
https://www.nhtsa.gov/sites/nhtsa.dot.gov/files/umtri-2016-8-wheelchairoccupantstudies.pdf .
ISO. ISO 7176-19:2008 + A1:2015. Wheelchairs-Wheeled Mobility Devices for Use as Seats in Motorvehicles . ISO, 2008.
Wij zien je wel.
Onderweg van overleven naar leven. Eindrapport en aanbevelingen werkgroep Wij zien je Wel. Wie zien je wel, maart 2020,
https://www.wijzienjewel.nl/producten/rapport-onderweg-van-overleven-naar-leven .
Songer, Thomas J., et al. The Injury Risk to Wheelchair Occupants Using Motor Vehicle Transportation . Sept. 2004, pp. 115–29.
“Travelling in Vehicles While in a Wheelchair: Joint Committee on Mobility for Disabled People.”
Physiotherapy , vol. 83, no. 6, June 1997, p. 305,
http://doi.org/10.1016/S0031-9406(05)66180-9 .
MBA, Karen L. Frost PhD, et al. “Wheeled Mobility Device Transportation Safety in Fixed Route and Demand-Responsive Public Transit Vehicles within the United States.”
Assistive Technology , vol. 24, no. 2, June 2012, pp. 87–101,
http://doi.org/10.1080/10400435.2012.659325 .
Mol, T. I., et al.
Kwaliteitsborging van extramurale medische hulpmiddelen: een rolverkenning van gebruikers van medische hulpmiddelen, zorgverzekeraars, gemeenten en de Inspectie voor de Gezondheidszorg en Jeugd. 2017, p. 44,
http://www.onderzoekpatientveiligheid.nl . ©2017 APH research Instituut.
MANUAL ON BORDERLINE AND CLASSIFICATION IN THE COMMUNITY REGULATORY FRAMEWORK FOR MEDICAL DEVICES . 2019.
MANUAL ON BORDERLINE AND CLASSIFICATION IN THE COMMUNITY REGULATORY FRAMEWORK FOR MEDICAL DEVICES . EUR, 2017.
Schotanus, Fredo, et al.
Handreiking Inkoop Hulpmiddelen. Geactualiseerde handreiking met afwegingen, uitdagingen en mogelijkheden voor gemeenten bij inkoop van Wmo-hulpmiddelen. VNG, 2018,
https://vng.nl/publicaties/handreiking-inkoop-hulpmiddelen-0 .
Peters, Chiel, et al. Handreiking Inkoop Hulpmiddelen. Afwegingen, uitdagingen en mogelijkheden voor gemeenten bij de inkoop van Wmo-hulpmiddelen. VNG, 0ktober 2014.
Ha, DongRan, et al. “Evaluation of Wheelchair Back Support Crashworthiness: Combination Wheelchair Back Support Surfaces and Attachment Hardware.”
Journal of Rehabilitation Research , vol. 36, no. 5, Oct. 2000, pp. 555–63,
https://pubmed.ncbi.nlm.nih.gov/12135653/ .
Plomp, Mr. M. J. “Kroniek concentratie controle.” Markt en Mededinging .
Heerdink, M. E. S.
Een Goede Zithouding, Dat Loont! Een Onderzoek Naar de Invloed van Een Anatomisch Verantwoorde En Stabiele Zitondersteuning Op de Kostenbesparingen in de Zorg. 7 July 2011,
https://essay.utwente.nl/62933/ .
Akerlof, George A., et al. De economie van list en bedrog . 2017.
Kok, L., et al. Kosten en baten van revalidatie . SEO, 2008.
Willemsen, Koen, et al. “Challenges in the Design and Regulatory Approval of 3D-Printed Surgical Implants: A Two-Case Series.”
The Lancet Digital Health , vol. 1, no. 4, Aug. 2019, pp. e163–71,
http://doi.org/10.1016/S2589-7500(19)30067-6 .
Zackowitz, Ilene B., and Alison G. Vredenburgh. “When Communication Failure Contributes to an Injury: A Case Study of Para-Transportation for Wheelchair Users.”
Proceedings of the Human Factors and Ergonomics Society Annual Meeting , vol. 51, no. 9, Oct. 2007, pp. 559–63,
http://doi.org/10.1177/154193120705100902 .
Priest, George L. “Strict Products Liability: The Original Intent.”
Cardozo Law Review , vol. 10, 1989 1988, p. 2301,
https://heinonline.org/HOL/Page?handle=hein.journals/cdozo10&id=2319&div=&collection= .
MSD, Peter J. Wolf, et al. “Wheelchair Tiedown and Occupant Restraint System Issues in the Real World and the Virtual World: Combining Qualitative and Quantitative Research Approaches.”
Assistive Technology , vol. 19, no. 4, Dec. 2007, pp. 188–99,
http://doi.org/10.1080/10400435.2007.10131876 .
Peters, A.
Code VVR 2019-2020 . A. Peters, 1 Jan. 2019,
http://codevvr.nl .
Kirby, R. L., et al. “Could Changes in the Wheelchair Delivery System Improve Safety?”
CMAJ: Canadian Medical Association Journal , vol. 153, no. 11, Dec. 1995, pp. 1585–91,
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1488010/ .
Samuel, Andrew, editor. “Cases of Product Liability.” The Winning Line: A Forensic Engineer’s Casebook , Springer, 2007, pp. 107–74, doi:10.1007/978-1-84628-097-9_3.
Keeton, Page. “Products Liability - The Nature and Extent of Strict Liability.”
University of Illinois Law Forum , vol. 1964, 1964, p. 693,
https://heinonline.org/HOL/Page?handle=hein.journals/unilllr1964&id=699&div=&collection= .
Cooper, Rory A. “A Perspective on the Ultralight Wheelchair Revolution.”
Technology and Disability , vol. 5, no. 3–4, Dec. 1996, pp. 383–92,
http://doi.org/10.3233/TAD-1996-53-419 .
“Wolturnus W5 ADL rolstoel.”
Double Performance ,
https://www.doubleperformance.nl/producten/adlrolstoelen/wolturnus-w5/ . Accessed 26 May 2020.
van Breukelen, Kees. “De ergonomische zit deel 2.”
Tijdschrift voor ergotherapie , 2010, p. 20,
https://dwarslaesie.nl/wp-content/uploads/2016/09/De-ergonomische-zit-Kees-van-Breukelen.pdf .
Markt, Autoriteit Consument &.
ACM Nordic Capital - Handicare concentratiebesluit | ACM.nl . 10 Dec. 2010,
https://www.acm.nl/nl/publicaties/publicatie/2507/Nordic-Capital---Handicare-concentratiebesluit .
Markt, Autoriteit Consument &.
Nordic Capital mag Conscia overnemen (concentratiebesluit) | ACM.nl . 22 Mar. 2019,
https://www.acm.nl/nl/publicaties/nordic-capital-mag-conscia-overnemen-concentratiebesluit .
VdTÜV.
Legal Compliance for the Transportation of Wheelchair Users Policy Document of the Roundtable “Safe Mobility for People with Disabilities.” VdTÜV, 1 Sept. 2013,
https://www.vdtuev.de/dok_view?oid=388608 .
Veenbaas, Roelof. TNO-rapport rolstoelvervoer.pdf . 03.OR.AC.048.1/ROV, TNO Wegtransportmiddelen, oktober 2003, p. 28.
AMF-Bruns. “Der Kraftknotenadapter | Personen- & Rollstuhlsicherung im Fahrzeug.”
Der Kraftknoten - Das Plus an Sicherheit ,
http://www.kraftknotenadapter.de/ . Accessed 24 May 2020.
Convenant samengesteld product . Firevaned, oktober 2017.
20100326 Study into Occupant Restraint Path in Custom Seating.Pdf . Coventry University, Faculty of Engineering, 26 Mar. 2010,
https://www.pmguk.co.uk/data/page_files/Best%20Practice/study%20into%20occupant%20restraint%20path%20in%20custom%20seating.pdf .
Kerncijfers zorgvervoer 2017 . Panteia, p. 10,
https://ai-mobiliteit.nl/ . Accessed 25 May 2020.
Aanbestedingsinstituut Mobiliteit .
https://ai-mobiliteit.nl/ . Accessed 25 May 2020.
Kirkels, A. F. Gehandicapten en ouderen deur-tot-deur vervoer . p. 45.
Buiren, Koert van, et al. De vloek van de winnende taxi: onderzoek naar het probleem van te lage biedingen bij aanbestedingen in het doelgroepenvervoer . 2016.